In his book, the pedagogy of oppressed, Freire calls traditional pedagogy the "banking model of education" because it treats the student as an empty vessel to be filled with knowledge, like a piggy bank. He argues that pedagogy should instead treat the learner as a co-creator of knowledge.
This was subsequently incorporated in the work of Augusto Boal in "theatre of oppressed" that is a form of "simulated education" where the audience learners (spect-actors) get to learn with the teachers (professional actors).
We often find simulations as an easy way of delivering medical education too and there are currently many tools and tactics to deliver these and yet most medical practitioners and practicing teachers tend to engage more with the primary beneficiaries of medical education (patients) in real time and perhaps even need their students and spect-actors to actually lend them a hand (as in a hands on approach to co-creating knowledge) and thus actually benefiting the primary beneficiaries of medical education, even creating a scope to correlate student and teacher learning outcomes with patient illness outcomes.
Co-creating emancipatory knowledge in real time:
We look back decades before "critical pedagogy" was founded and peer into the life of an Indian hands on Marxist anarchist revolutionary, Bhagat Singh, who for some time in his short existence of 20 years had been exploiting the power of drama as a means to inspire the revolt against the British, purchasing a magic lantern to show slides that enlivened his talks about revolutionaries.
In 1929, he proposed a dramatic act to the HSRA intended to gain massive publicity for their aims. Influenced by Auguste Vaillant, a French anarchist who had bombed the Chamber of Deputies in Paris,[36] Singh's plan was to explode a bomb inside the Central Legislative Assembly. The actual intention was for the perpetrators to allow themselves to be arrested so that they could use court appearances as a stage to publicise their cause. The Supreme Court of India established a museum to display landmarks in the history of India's judicial system, displaying records of some historic trials. The first exhibition that was organised was the Trial of Bhagat Singh.
Much has happened in the years since then with further evolution of critical pedagogy embracing critical realism that allows healthcare learners to 1) understanding complex outcomes, (2) optimizing interventions, and (3) researching biopsychosocial pathways. Such questions are central to evidence-based practice, chronic disease management, and population health.
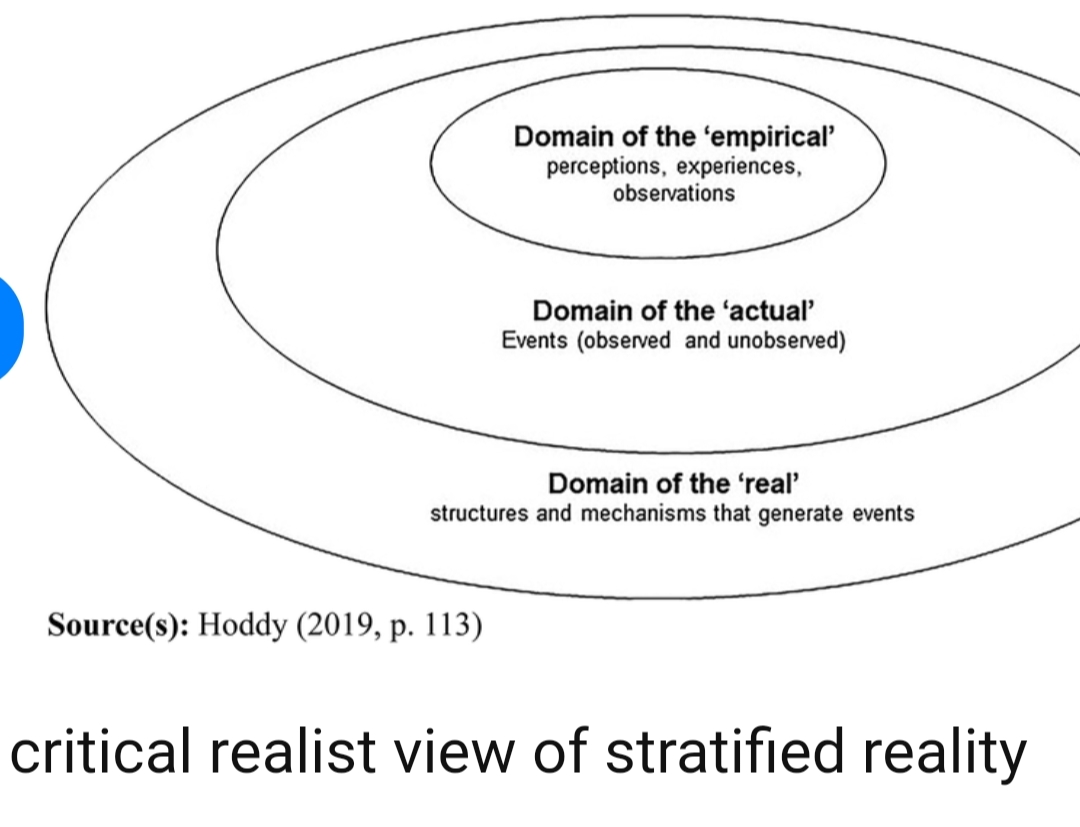
While we don't have a ©️ on the very useful figure of critical realist view of stratified reality shared by Hoddy et al : Source: https://www.
we would like to add our own diagram as a positive contribution to expand on their viewpoint from a medical cognition lens and the essence of it is all about the individual patient's and physician's cognition at the centre of the concentric circles corresponding to Hoddy's domain of the 'empirical' as in perceptions, experiences and observations of 'individual cognition' while the surrounding concentric circle forms a ring of 'actual collective cognition' that tries to tie together all knowledge elements into an 'ontology' many of which are unknown and form the connecting link to the next ring which is Hoddy's domain of the 'real' that contains all the structures and mechanisms that generate events that again feed back cyclically into the central concentric circle of individual perception of empirical events surrounded by the ring of collective cognitive interpretation of 'actual' events.


In our CBBLE and PaJR groups we witness daily in real time, a co creation of user driven learning community ontologies powered by Web 2.0 critical realist heutagogy through team based learning between multiple stakeholders such as health professional learners, faculty, patients and their relatives that is increasingly supported by Web 3.0 technology where all these stakeholders co create as online system users, with a username, something that has been labelled in the past user driven healthcare.
Ref 35: https://pubmed.ncbi.nlm.
This co creation has enabled healthcare educator practitioners to not only remain focused on real patient care centred learning outcomes but develop realist ontologies for medical education and practice such as "real patient OSCEs" that retain whole patient clinical complexity rather than reduce it to smaller parts in order to optimize clinical complexity.
Full text: https://fenix.iseg.ulisboa.pt/downloadFile/281608120804971/Critical%20realism%20and%20GT%20Hoddy%202019.pdf
Present failure:
"Many if not most students come to the university in order to gain access to and eventual enfranchisement in 'the establishment,' not to critique and reject its privileges."
Students want to gain, rather than to critique, positions of privilege, as encouraged by critical pedagogues."
Updated terminology:
[06/11, 09:50] Kmcq: Heutagogy!
Pedagogy is outdated
[06/11, 09:52]: It's a heutagogist's strategy of calling heutagogy as pedagogy but yes I realise it would be better to name it heutagogy
@Meta AI how's heutagogy different from pedagogy?
[06/11, 09:53] Meta AI: Heutagogy and pedagogy are two distinct approaches to learning and teaching:
*Pedagogy:*
1. Teacher-centered
2. Focus on transmitting knowledge
3. Emphasis on instructor's expertise
4. Learners receive information passively
5. Assessment-focused
*Heutagogy:*
1. Learner-centered
2. Focus on self-directed learning
3. Emphasis on learner's autonomy
4. Encourages critical thinking, reflection, and meta-cognition
5. Flexibility and adaptability
Key differences:
1. Control: Pedagogy (teacher) vs. Heutagogy (learner)
2. Focus: Knowledge transmission (pedagogy) vs. Learning process (heutagogy)
3. Role of teacher: Expert (pedagogy) vs. Facilitator/Mentor (heutagogy)
Heutagogy fosters:
1. Self-directed learning
2. Personalized learning paths
3. Collaboration
4. Real-world applications
5. Reflection and meta-cognition
In heutagogy, learners take ownership of their learning, and teachers guide and support.
*Evolution of learning approaches:*
1. Pedagogy → Andragogy (adult learning) → Heutagogy (self-determined learning)
*Implications for education:*
1. Shift from standardized to personalized learning
2. Emphasis on developing critical thinking, creativity, and problem-solving skills
3. Integration of technology-enhanced learning
4. Redefining teacher roles and responsibilities
Collective cognition feedback Update:
[08/11, 08:51]drnr : It may be difficult for medical teachers to emulate Bhagat Singh's dramatisation: to allow or kill a patient for explaining the natural history of the disease, and then face the fury of the family, the MCI and the never ending judicial proceedings!
The medical student may not be left with many teachers, unless Hezbollah takes over medical education ((strictly for boys (pun intended))!
[08/11, 08:55]rb: That was an extreme case!😅
[08/11, 08:56]rb: But because of some Western Bhagat Singh's who cleverly designed the randomized controlled trial post pencillin, we can still reap it's benefits
[08/11, 08:59]drnr: You could always have a new GCP, with a slave act enabled
[08/11, 09:07]rb: The existing ones are just that! Slave acts! Yes that's the term to best describe most guideline based medicine vs true evidence based medicine 👏👏
[08/11, 09:10] rb: This makes me reimagine the randomized controlled trial participant as Bhagat Singh on trial (and to be true to medical ethics and patient autonomy, the patient has had a good role in it's design) although it's difficult to predict the random outcome for any of the participants in the trial as that's what equipoise should be all about! The patient Bhagat Singh just stands there, brave and strong ready to meet whatever the dice ordains!
No comments:
Post a Comment