Current Project PI: Dr Haripriya
Project details from her portfolio:
Similar project quantitative analysis with question to PI and project team:
Check out the quantitative thematic analysis in the form of various demographic and disease related themes (as quantitative associations with patients of altered sensorium) from a past similar project from Osmania shared full text here 👇
Share if you can answer the following questions quickly after reading the above quantitative thematic analysis:
What was already known to you around altered sensorium outcomes before your study?
What was already known to the world around altered sensorium outcomes before your study although you didn't know it?
What was not known to the world around altered sensorium outcomes before your study?
Current Project qualitative analysis:
1) First case case report form and thematic analysis:
2) Second case report form and thematic analysis:
2nd case report form rough draft of "altered sensorium ProJ" patient for thematic analysis in the ProJR as shared by the PI Dr Haripriya:
Data below retrieved from the hospital
Diagnosis? NEUROTOXOPLASMOSIS.? NEUROTUBERCULOSIS.
Case History and Clinical Findings
PRIMARY SURVEY:PR:108 BPMBP:130/90 MM/HG
RR:22CPM
TEMP: 103F.
SPO2:98% AT RBS:113MG/DL
CHIEF COMPLAINTS:Patient has complaints of generalised weakness since 1 week.h/o loss of speech and deviation of mouth since 3 days
HOPI: PATIENT WAS BROUGHT TO CASUALITY WITH COMPLAINTS OF GENERALIZED WEAKNESS OF BOTH UPPER AND LOWER LIMBS SINCE 1 WEEK, COMPLAINTS OF UNABLE TO SPEAK SINCE 3 DAYS , COMPLAINTS OF DEVIATION OF MOUTH TO RIGHT SIDE SINCE 3DAYS , COMPLAINTS OF FEVER SINCE 1 DAY.NO HISTORY OF SEIZURES,HEADACHE, GIDDINESS,SHORTNESS OF BREATH,FEVER,RASHES,PAIN ABDOMEN AND BURNING MICTURATION.
SECONDARY SURVEY:
GENERAL:PATIENT IS DROWSY, NON COHERENT , NOT ORIENTED TO TIME, PLACE AND PERSON.
HEAD: ATRAUMATIC, NORMOCEPHALIC ,
GCS: E2V2M4[8/15]EYES: ATRAUMATIC, NO DISCHARGE, B/L PUPILS EQUAL REACTING TO LIGHT,
RT EYECATARACT.EARS:ATRAUMATIC, NO DISCHARGE.NOSE:ATRAUMATIC, NO DISCHARGE.NECK:NO NECK SWELLINGS,NO JVP DISTENSION,B/L CAROTIDS FELT, NO STRIDOR CHEST: B/L CHEST RISE EQUAL.HEART: S1 S2 HEARD, NO MURMURS.LUNGS: BAE+ No added breath sounds.ABDOMEN: SOFT,NON TENDER,NO DISTENSION,BOWEL SOUNDS PRESENT
PAST MEDICAL HISTORY: nil significant
PAST SURGICAL HISTORY : no past surgical history
NO SIGNIFICANT FAMILY HISTORY
NO KNOWN DRUG OR FOOD ALLERGIES NO KNOWN
COMORBIDITIES.
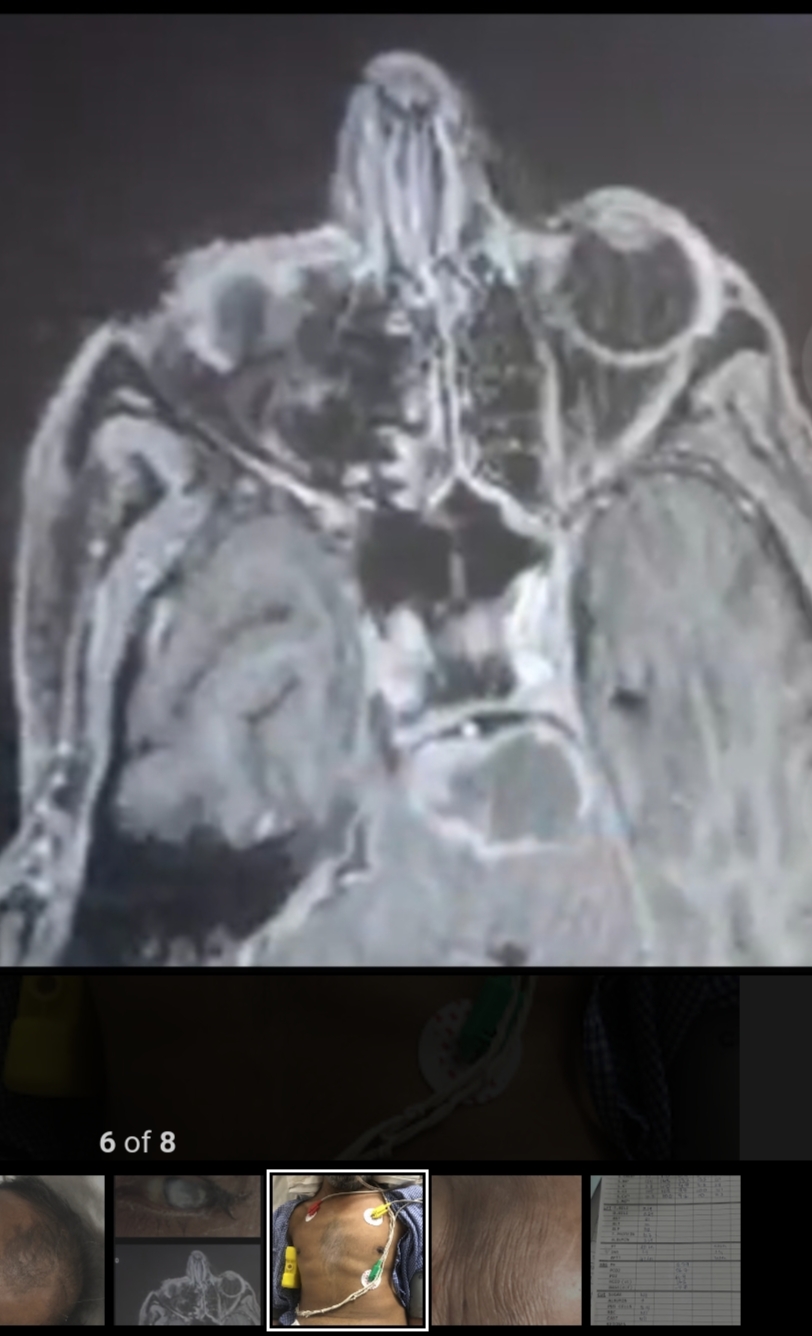
Investigation MRI BRAIN PLAIN AND CONTRAST:Multiple ring enhancing lesions in pons mid brain bilateral straito capsular regions,left frontal lobe andright cerebellar hemisphere with extensive edema in the above areas.F/S/O Neurotoxoplasmosis/
CSF ANALYSIS:
CSF CULTURE:zn stain-no acid fast bacilli seen. gram stain:few disintegrated pus cells,occasional gram positive cocci in pairs seen.CSF CYTOLOGY:few lymophocytes and few monocytes are seen.
Treatment Given(Enter only Generic Name)1)INJ NEOMOL 1GM IV/TID
2)INJ PANTAPRAZOLE 4OMG IV/STAT
3).INJ.ONDENSETRON 4MG IV/OD
4)OPTINEURON 4AMP IN 500ML NS IV/OD
5)TAB ECOSPORIN 75MG/RT/OD
6)TAB ROSUVASTATIN 40MG/RT/OD
7)INJ CLEXANE 60MG/SC/OD
8)INJ MANNITOL 100 /IV/TID
9)INJ LEVETIRACETAM 500MG /IV/BD
10)INJ THIAMINE 200MG /IV IN 500ML/NS/Od
11)TAB FOLIC ACID 5MG/RT/OD
12)TAB DOLUTGRAVIR 5OMG/OD+TAB LAMIVUDINE 300MG+TENOFOVIR 300MG
13)TAB SULFADIAZINE 1GM/RT/6TH HOURLY
14)TAB PYRIMETHAMINE 50MG/RT/6TH HOURLY
15)TAB LEUCOVORIN 15MG/RT/6TH HOURLY
Advice at Discharge
1)TAB DOLUTEGRAVIR 5OMG/OD+TAB LAMIVUDINE 300MG+TENOFOVIR 300MG OD FOR 1MONTH
2)TAB SULFADIAZINE 1GM/RT/6TH HOURLY FOR 1 MONTH
3)TAB PYRIMETHAMINE 50MG/RT/6TH HOURLY FOR 1 MONTH
4)TAB LEUCOVORIN 15MG/RT/6TH HOURLY FOR 1 MONTH5]TAB.PANTAPRAZOLE 40MG RT/OD FOR 1 MONTH6]TAB. MVT RT/OD
When to Obtain Urgent CareIN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR
ATTEND EMERGENCY DEPARTMENT.Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER SIGNATURE OF PG/INTERNEE SIGNATURE OF ADMINISTRATOR. SIGNATURE OF FACULTY
Discharge Date:25/09/23 Ward:EMD
19/09/23, 21:11 - Messages and calls are end-to-end encrypted. No one outside of this chat, not even the App, can read or listen to them. Tap to learn more.
19/09/23, 19:03 - Haripriya Maam Kims Pg created group "52M with altered sensorium secondary to HIV encephalopathy and toxoplasma Telangana PaJR"
19/09/23, 21:11 - Intern who drafted the PaJR discussion joined using this group's invite link
19/09/23, 21:14 - +91 9 joined using this group's invite link
19/09/23, 21:31 - +91 joined using this group's invite link
19/09/23, 22:08 - +91 joined using this group's invite link
19/09/23, 22:54 - +91 joined using this group's invite link
20/09/23, 07:53 - Sai charan Sir GM Pg Kims joined using this group's invite link
22/09/23, 19:31 ALLM : His gcs has improved
He has eye opening to verbal commands from today morning.
Previous his fever was always a 101-103 now it has touched down to 100 from morning sir.
Patient has improved clinically and they are also planning for his discharge on monday.
23/09/23, 16:16 - Haripriya Maam Pg: His GCS is E3V1M1 sir
Fever spikes decreased(99F)
Csf analysis didn't showed any cells sir
Wasn't send for Indian ink stain sir
23/09/23, 16:37 ALLM : Update and discuss his treatment asap
Also are you evaluating most of your altered sensorium patients with Glasgow scale only!!
What about MSE?
Please see here how our previous PGs had evaluated altered sensorium using GCS as well as other scales
At least by reading it you will realize how a PG presentation should be like?
Who's presenting this patient in the Thursday clinical meeting among your other thesis cases? I shall request Prof Maruthi Sharma to also share his experiences
Please share the treatment plan asap and readmit the patient with us after discharge by the other department who admitted him as an emergency.
23/09/23, 16:38 ALLM : Fever chart?
11/10/23, 17:50 - +91 joined using this group's invite link
11/10/23, 17:54 - +91 joined using this group's invite link
11/10/23, 18:08 - Rakshitha Kim's Intern joined using this group's invite link
11/10/23, 18:10 - +91 joined using this group's invite link
11/10/23, 18:29 - Dr Durga Krishna Sir Pg joined using this group's invite link
11/10/23, 18:38 - +91 joined using this group's invite link
11/10/23, 20:47 - Manasa Maam Kims Med Pg joined using this group's invite link
11/10/23, 22:06 joined using this group's invite link.
June 2024 Thematic analysis steps:
Step 1:
Case 2 step 1 of qualitative thematic analysis by project PI:
Socratic questioning around the case 2 initiated by PI:
1) What is the cause for the seizure episode initially During presentation in 2008??
2) When he got tested with RVD Positive for the first time,is it RVD itself or RVD induced vasculitis leading to seizures?
3)The acute history in the current admission??
Is it the HIV encephalopathy responsible for his altered sensorium,if yes why is the history so short,if it's encephalopathy,or if it's the superadded infection causing his worsening sensorium??
Welcome inputs and socratic questioning by other team members
[27/06, 12:37] Sai Charan 2020: Patient is having altered sensorium with FND..?
Power 3/5 ..? Hemiparesis or Quadriparesis..?
Nothing detailed about clinical localisation.
MRI - subacute infarct vs SOL infective vs malignancy - how was this ruled in or out..? Based on radiology alone..? If so what is the sensitivity of MRI in differentiating infective SOL vs Neoplastic SOL..?
CSF cytology - few lymp and mono cytes seen..? Normal or abnormal ..? Nothing mentioned in case report
[27/06, 12:40] Sai Charan 2020: Known facts :
Altered sensorium in CVA and SOL is globally known
Unknown :
Is this altered sensorium and FND attributed to SOL or CVA..?
What triggered his seizures..?
Surely not meningitis ( if csf normal )
Can subacute infarct be the cause for Seizures..?
[27/06, 13:58] group moderator: 👆@Sai Charan 2020 Also try the questions here in the context of the entire quantitative thematic analysis from Osmania
[28/06, 10:08] group moderator: Inputs on case 2 for thematic analysis today shared by project PI:
[28/06, 08:31] Pushed Communicator 1N21: Yes sir the infective foci is causing FND(as there is deviation of mouth)In this patient.
And the 3/5power, is the patient is in altered sensorium and the power couldn't be elicited sir,so as the patient is moving the limbs against gravity to deep pain the power is taken as 3/5..
On MRI,with such an acute history of 1 week,it's most likely going towards vascular/infective etiology rather than malignancy (Taking a chronic course)
Rather than MRI alone the clinical findings are also taken into consideration,that is if it's vascular origin involving cerebral Cortex the area of involvement will be very huge to produce hemi/Quadriparesis ,even if it may miss initially in MRI, after 1 week it could be seen after 1 week of imaging..
And the fever(could also be seen in central cause,central fever),but in the background of immununocomprimised infection could be mostly considered..
CSF cytology:.No atypical cells,and Total count is 150cells,lymphocytic predominant,with elevated protein and normal glucose sir,mostly going towards Fungal etiology sir ..
[28/06, 08:31] Pushed Communicator 1N21: Patient is having altered sensorium with FND..?
Power 3/5 ..? Hemiparesis or Quadreparesis..?
Nothing detailed about clinical localisation.
MRI - subacute infarct vs SOL infective vs malignancy - how was this ruled in or out..? Based on radiology alone..? If so what is the sensitivity of MRI in differentiating infective SOL vs Neoplastic SOL..?
CSF cytology - few lymp and mono cytes seen..? Normal or abnormal ..? Nothing mentioned in case report
[28/06, 10:51] Chandana 2020 SR: MRI PLAIN-
E/o hyperintense signal on DWI/FLAIR / ADC noted on b/l corona radiata b/l genu of ant corpus collasum b/l thalamus b/l basal ganglia b/l midbrain pons and b/l cerebellar peduncles and b/l frontal regions
Features suggestive of Subacute infracts
MRI CONTRAST-
Multiple ring enhancing lesions in pons midbrain b/l striatocapsular regions left frontal lobe and rt cerebellar hemisphere with extensive edema in the above areas
f/s/o Neurotoxoplasmosis/Neurotuberculosis
Does this mean the lesions are reported as subacute infarcts on plain MRI and on repeating with contrast it was reported as toxoplasmosis?
Because sub acute infarct vs toxoplasmosis with edema can be difficult to differentiate without contrast.
But the number and location of lesions with risk factor pointing it more towards toxo/TB.
In that case there are no infarcts.
Images of MRI would be helpful if any available.
[28/06, 11:00] Rakesh Biswas: Good point on resolving diagnostic uncertainty to optimise clinical complexity
If you check out the case 1 link and the emerging themes from it encoded there, we may realise there's a pattern in our clinical cognition thematic analysis where we identify
Themes around diagnostic uncertainty
Themes around therapeutic uncertainty
in most of our cases and then conclude what we learned that we as well as the world didn't know earlier
[28/06, 11:21] Chandana 2020 SR: Resolving therapeutic uncertainty can be possible only with good follow up and data related to recovery
[28/06, 11:26] Rakesh Biswas: That's a great learning point identified
I would classify it as something already known but globally not known to that extent and would be a valuable contribution from our thesis around developing robust follow up systems that also emerged as pointed out by an LLM shared by @Sai Charan Kulkarni 2020 KIMS Pg and all archived in case 1 blog
[28/06, 21:55] Rakesh Biswas: Inputs from our principal investigator PI for this project:
[28/06, 21:25] Pushed Communicator 1N21: Themes emerging:
Unmarried Middle aged man with altered sensorium
Clinical complexities:
RVD in Young age with opportunistic infections with FND
Diagnostic uncertainty:
Focal deficits could be ? secondary to Subacute infarct/Infection/neoplasms
Therapeutic uncertainty:
What to treat??
Infarct vs Infection
[28/06, 21:50] ALLM: So what was the unit's diagnosis and therapy offered?
[28/06, 21:57] group moderator: @Chandana KIMS 2020 SR @Sai Charan Kulkarni 2020 KIMS Pg if you compare the diagnostic and therapeutic uncertainty of case 2 with case 1, which do you think has higher uncertainty?
[28/06, 22:00] group moderator: The other general assumption that is getting traction here is that therapeutic uncertainty need not necessarily correlate with diagnostic uncertainty as medical teams generally tend to treat whatever differentials exist that are treatable, which in most cases would involve inflammation due to either infection or immune response.
[28/06, 22:30] Sai Charan 2020: To me both cases have uncertainties.. probably I am not expertise enough to prioritise uncertainties. But at macro level Diagnostic uncertainty(DU) in case 1 is pinch of salt high than case 2.
In case 2 the only DU is between infection, thrombotic or neoplastic where first 2 can be self healed by body defence mechanism against insult. But neoplastic would need some specialised intervention.
Where as case 1, why fluctuating sensorium ( sensorium improved despite of urea going down & corrected hypoxia ).
Cause of Dementia since 2-3 months ..?
Radiological findings..? If subacute or small vessel Ischemic changes. Then we have a lead both small vessels of heart and brain involved. Micro vascular changes may be due to adipokine mediated ( speculative ).
No comments:
Post a Comment