04/02/23, 10:50 - ~
� created group "88F - CAD Cerebral infarct hyponatremia recovered from ventilator"
21/02/23, 12:54 - H joined using this group's invite link
21/02/23, 12:54 - Dr Vamshi Pg Gmed2 joined using this group's invite link
21/02/23, 12:54 - Dr Vinay Pg Gmed 2 joined using this group's invite link
21/02/23, 12:55 - Dr Durga Krishna Pg Med2 joined using this group's invite link
21/02/23, 12:56 - Dr Shashikala Pg Med joined using this group's invite link
21/02/23, 12:58 - Dr Shashikala Pg Med:
PaJR soap updates
Patient currently in Icu
Unit1
S:
Stools not passed
Fever spike 101 f @ 2am
O:
O/E: conscious coherent and oriented to place
Temp- 98f
Bp-80/40 mmhg on NORAD 12 ml/hr and DOBUT 9ml/hr
Pr- 106 bpm
Rr-20cpm
Spo2-96 % on 2l oxygen
Grbs: 97mg/dl
Systemic Examination:
Cardiovascular System : S1, S2 heard, palpable p2 +
Respiratory System : decreased air entry on rt side
AA Crepts positive on left side
Central Nervous System : patient is oriented to place
E4v5m6
Per abdomen : soft, 4/min
A:
ALTERED SENSORIUM secondary to ?UREMIC ENCEPHALOPATHY
HYPOXIC ENCEPHALOPATHY WITH HEART FAILURE WITH MIDRANGE EJECTION FRACTION(EF 42%)
SECONDARY TO ANTERIOR WALL MI
WITH HYPERKALEMIA SECONDARY TO INCREASED INTAKE OR KIDNEY INJURY
WITH ILD WITH L. LOWER-LOBE CONSOLIDATION with URETHRAL CARUNCLE
WITH G1 BED SORE
P:
1. 200ml milk 4th hourly
2. 100ml water 4 th hourly
3. Inj. NORAD 14mg in 46 ml ns @1 ml/hr ( increase or decrease to maintain MAP OF 55 mmhg
4. Inj DOBUTAMINE 250mg in 50ml NS @ 8 ml/hr
5. T. Carvidolol 3.125 mg/Rt/OD
6. INJ. Ceftriaxone 1gm/iv/bd
7. Inj. LASIX 40mg BD/IV/BD(if sbp> 110 without narad support
8. T. ECOSPIRIN 75/75/10 mg rt OD
9. Neb with IPRAVENT TID
10. T.NODOSIS 500mg iv bd
11. O2 inhalation to maintain spo2 >94
12. Monitor vitals
25/02/23, 16:47 - Dr Rakesh Biswas Sir HOD added Dr Ajay Gen Med Pg
25/02/23, 16:50 - Dr Rakesh Biswas Sir HOD: EF is around 30%
It's likely that she had a PRES
@ team member@ team member@team member@team member
In the context of this patient who presented with recurrent altered sensorium can you review the literature around similar presentations in PRES
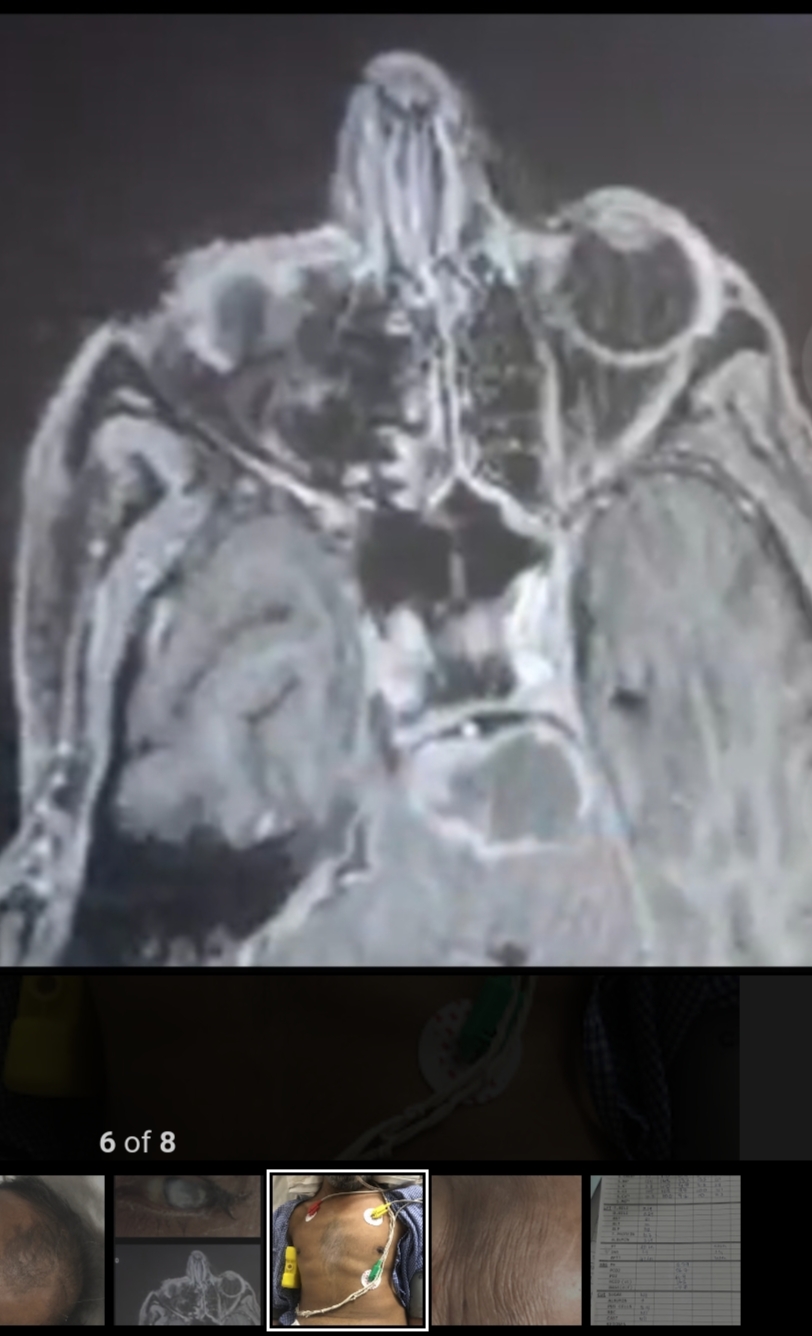
Anything in her radiology to suggest that? Is the posterior cerebral structure more commonly involved in PRES? If yes why?
25/02/23, 18:46 - Dr.Deepika Ch:
Here's a detailed history of the patient's event timeline:
88 year old female
Her daily routine-
A joyful 88 year old female starts her day at 6am with a cup of tea/ coffee and then she does her routines like cleaning the house, cooking
Has her breakfast at 9 to 10am which is cooked by herself
She then takes rest while watching TV or even talking to her neighbours
Lunch at around 2 pm which most of the time is rice,Dal and some curry
She then tries to relax herself and find pleasure in talking to her neighbours in the porch for which she even refused to stay at her sons house 🏠
Cooks her own food and goes to sleep at around 9pm
This routine of her continued till 6 months back then
She developed disturbances in her behaviour with increased irritability , decreased interaction with people
Slowly later there is increased self talk
4 months back on one fine day patient was found walking towards the opposite village at night ,neighbours recognising her have informed the family and made her stay overnight ,she was slightly agitated and irritable saying she was heading to village to get her debts back from the people she has given to.
2months back patient remained more or less the same mentally ,then she had increased forgetfulness
Often started forgetting to turnoff the gasstove,switching off lights/fans, close the doors
She developed involuntary movements of limbs (upperlimbs) which were on and off (no seizure like activity),altered sensorium and was taken to local practioner ,neuroimaging(ct) was done and found to be normal which resolved after 2-3 days but involuntary movements didn't subside though decreased intensity
Patient had an episode of weakness of lowerlimbs ,Inability to walk her son being local practioner got investigated for Hypokalemia found to have K-2.0 and was added dietary supplementation and syp potchlor
1month back February 1st week patient had shortness of breath ,altered sensorium and brought to our hospital and treated heartfailure, hyponatremia.patient sensorium improved and was stable during discharge
10days back patient developed similar episode and got investigated outside and found to have ?ILD on hrct
Patient then was brought here for further management .
25/02/23, 21:30 - Dr Haripriya Pg: Sir can be think it as PRES
As we are not sure about her vision disturbance
And no seizures
And basically as PRES is a clinicoradiological diagnosis
We are not having radiological evidence and in PRES there is refractory headache which is not present in this patient
And she is having fluctuating sensorium,and I think PRES wont develop such fluctuations in sensorium
As in previous admission she is having Ef of 30%,and her sensorium improved at admission,and with the same Ef was normal for 20 days..
25/02/23, 21:45 - Dr Saicharan Pg Gmed2: Good thought process 👏🏻👏🏻
Given her clinical condition with fluctuating sensorium PRES is a good possibility but can it happen with normal blood pressure...? @919704090596 i think her admission bp is normal..
The paradox here is initially we also thought altered sensorium is due to hypoxia and uremic but even after hypoxia correction her sensorium not improved and surprisingly her sensorium improved ( though not completely normal ) even after worsened urea ( from 102 to 160 ) pointing less possibility of Uremic encephalopathy..!!
@team member : Good thesis case to be included in your thesis.. also look into other causes too
25/02/23, 21:51 - Dr.Deepika Ch: Sir how come it not be her neurodegenerative condition which could have worsened acutely
( acute stress condition )
As I could see her condition in toto which isn't normal even prior to this episode
Others too (uremia,hypoxemia)which could have added to her already affected brain/ sensorium?!
25/02/23, 21:55 - Dr Haripriya Pg: What u think is the stressor
25/02/23, 22:00 - Dr.Deepika Ch: Any stressor like
Hypoxemia 2° to heart failure,uremia,infections,MI...
25/02/23, 22:08 - Dr Haripriya Pg: She is having reduced EF since 1 month and uremia we are not sure about the urea levels at her home,bcz now her urea is 150 and she is oriented
And infections,not at all
She is having fever just bcz of thromboprophylaxis
25/02/23, 22:09 - Dr Haripriya Pg: Thrombophlebitis *
25/02/23, 22:10 - Dr Haripriya Pg: MI she is having since last admission
25/02/23, 22:16 - Dr Saicharan Pg Gmed2: @team member , as you are altered sensorium specialist what about your thoughts on Neurodegenerative condition leading to her altered sensorium..??
25/02/23, 22:18 - Dr.Deepika Ch: How sure are we regarding her prior status!
Agreed we r not sure of the trigger
Her changes in sensorium were from past few months which couldn't be explained by the uremia,hypoxia!( as it was normal ?!)
25/02/23, 22:20 - Dr Saicharan Pg Gmed2: What wasn't normal when you saw her in toto in her previous history....?? Can you elaborate on this please
25/02/23, 22:36 - Dr Haripriya Pg: Am sure regarding her sensorium😊
25/02/23, 22:49 - Dr.Deepika Ch: In sense the cause??
25/02/23, 23:31 - Dr Rakesh Biswas Sir HOD: What radiologic evidence is lacking for PRES?
What is the cerebrovascular pathology in PRES?
It appears to be cerebral vasculopathy also mimicking a neurodegenerative disorder @team member?
25/02/23, 23:36 - Dr Haripriya Pg: Neurodegenerative disorder
Is it waxing and waning sir
25/02/23, 23:37 - Dr Rakesh Biswas Sir HOD: Can be due to other factors. Check out the patient descriptions in @team members's last publication
25/02/23, 23:37 - Dr Haripriya Pg: Okay sir
27/02/23, 17:02 - Dr.Deepika Ch: Yes sir
27/02/23, 17:06 - Dr Saicharan Pg Gmed2: Please share the literature about PRES occuring with normal blood pressure ( age adjusted normal BP )...?
27/02/23, 19:22 - Dr Rakesh Biswas Sir HOD added Dr Prachethan Jr Gmed
27/02/23, 19:23 - Dr Rakesh Biswas Sir HOD changed the group description
27/02/23, 19:25 - Dr Rakesh Biswas Sir HOD added Dr Himaja Jr Gmed
27/02/23, 19:23 - Dr Rakesh Biswas Sir HOD: @tm @tm Please share today's trend-chart soap update for this and every ICU AMC patient asap
27/02/23, 19:26 - Dr Rakesh Biswas Sir HOD changed the group name from "88F - CAD Cerebral infarct hyponatremia recovered from ventilator" to "88F CAD Cardiogenic shock Cerebral infarct hyponatremia altered sensorium Telengana PaJR"
27/02/23, 19:24 - Dr Rakesh Biswas Sir HOD changed the group description
27/02/23, 19:30 - Dr Rakesh Biswas Sir HOD: Also I think we shouldn't share clinical breast images of women unless absolutely necessary so please review that and crop or take with appropriate gown
27/02/23, 19:37 - Dr Rakesh Biswas Sir HOD changed this group's icon
27/02/23, 19:33 - Dr Rakesh Biswas Sir HOD: IMG-20230227-WA0079.jpg (file attached)
27/02/23, 19:35 - Dr Rakesh Biswas Sir HOD: IMG-20230227-WA0080.jpg (file attached)
27/02/23, 19:36 - Dr Rakesh Biswas Sir HOD: Another fever chart dated 3/2/23 uploaded by Manaswini (add her to this group) shows identifiers. Ask to remove asap @tm @tm
27/02/23, 19:45 - +91 96768 24264 joined using this group's invite link
27/02/23, 19:45 - Dr. Dinesh Datta joined using this group's invite link
27/02/23, 20:04 - Dr Navya Gen Med Pg joined using this group's invite link
27/02/23, 20:16 - Dr.Deepika Ch: Commonly, PRES evolves over a matter of hours, with the most common presenting symptoms being seizures, disturbed vision, headache, and altered mental state (4) (Figure 1). More than 70% of patients with PRES are hypertensive, though a significant proportion have normal or only mildly raised blood pressure (3-7).
trigger is usually identifiable—most commonly, acute hypertension—but patients often have other comorbidities that may predispose them to developing PRES. Peak systolic blood pressure is usually between 170 mmHg and 190 mmHg (2,4), but 10% - 30% of patients have normal or only mildly elevated blood pressure (2,4). In PRES, the causes of acute hypertension are commonly acute kidney injury or eclampsia (3,4), but hypertension is also reported in cases of autonomic disturbance, for example Guillain-Barré syndrome (10,11), and after illicit drug use
27/02/23, 20:18 - Dr Rakesh Biswas Sir HOD: 👆Answer first two @tm
27/02/23, 20:20 - Dr.Deepika Ch: The exact pathophysiological mechanism of PRES is still unclear. Three hypotheses have been proposed till now, which include (i) Cerebral vasoconstriction causing subsequent infarcts in the brain, (ii) Failure of cerebral autoregulation with vasogenic edema, and (iii) Endothelial damage with blood–brain barrier disruption further leading to fluid and protein transudation in the brain. The distinct imaging patterns in PRES are represented in Table Table22 [5]. The reversible nature of PRES has been challenged recently based on new reports of permanent neurological impairment and mortality reaching 15%.
hypertension associated or drug-induced PRES, the effective therapy includes withdrawal of offending agent, immediate control of blood pressure, anti-convulsive therapy and temporary renal replacement therapy (hemodialysis/peritoneal dialysis) if required. In Systemic lupus erythematosus-related PRES, aggressive treatment with corticosteroids and cyclophosphamide is effective. Corticosteroids may improve vasogenic edema, but there is no solid evidence for usage in PRES.
01/03/23, 18:53 -Patient advocate: Dear Dr. Rakesh sir & Dr. Mohd Zain sir and team (all PG's and Interns), I wanted to express my deepest gratitude for the exceptional care you provided to my mother during her recent treatment. Your expertise, compassion, and dedication were truly remarkable, and our family is forever grateful for your hard work and commitment to her health. Thank you from the bottom of our hearts.
***********************************************************************************
From
01/03/23, 19:00 - Dr Saicharan Pg Gmed2: Thank you.
01/03/23, 19:01 - Dr Saicharan Pg Gmed2: Please don't forget to share her daily updates here
01/03/23, 19:05 Patient advocate: Sure Sir
01/03/23, 19:13 - Dr Saicharan Pg Gmed2: Please don't share patient identifiers in the public domain.
01/03/23, 19:13 - Dr Saicharan Pg Gmed2: This is to maintain patient privacy and confidentiality..
01/03/23, 19:24 -Patient advocate: Ok Sir
Discharge summary of the first admission from Feb 3 to Feb 8 2023:
Finally the patient was discharged after a stay of 5 days and while intern Dr Gana Prasad typed the discharge summary, it was guided by residents Dr Haripriya and Dr Chandana. The caps lock is a feature of the hospital EMR that is currently limited to billing and discharge summaries print out production. The PaJR discussion pasted above is where the actual core EHR content and insights for thematic analysis takes shape.
DEPARTMENT OF GENERAL-MEDICINE
DISCHARGE SUMMARY of the first admission
Pay Type : Paying
Age/Gender : 86 Years/Female
Address :
Discharge Type: Relieved
Admission Date: 03/02/2023 12:13 AM
Diagnosis at discharge:
HEART FAILURE WITH REDUCED EJECTION FRACTION SECONDARY TO CORONARY
ARTERY DISEASE(EF 30%) WITH ANTERIOR WALL MI WITH TRUE HYPONATREMIA
SECONDARY TO SIADH(RESOLVED) AND HYPOKALEMIA (RESOLVED) WITH BILATERAL
LUNG CONSOLIDATION
Case History and Clinical Findings
COMPLAINTS OF Irrelevant TALK AND Altered MENTAL STATUS SINCE 10 DAYS
COMPLAINTS OF SHORTNESS OF BREATH SINCE 3 DAYS
COMPLIANTS OF COUGH SINCE 3 DAYS
HOPI:
PATIENT WAS APPARENTLY ASYMPTOMATIC 10 DAYS AGO AND THEN SHE DEVELOPED
ALTERED MENTAL STATUS ON AND OFF AND HER SPEECH WAS INCOHERENT AT TIMES
AND BECOMING NORMAL ON HER OWN.
EACH EPISODE LASTED 10 MINS
Page-2
COUGH WAS PRODUCTIVE TYPE 2 DAYS AGO WITH WHITE SPUTUM'MUCOID CONSISTENCY
AND SCANTY IN AMOUNT , NOW IT IS OF DRY TYPE
SHE ALSO HAD SHORTNESS OF BREATH WHICH WAS GRADE III INITILLY AND THEN
PROGRESED TO GRADE IV FOR WHICH SHE WENT TO LOCAL HOSPITAL AND ECHO WAS
DONE- CAD (LAD TERRITORY) GLOBAL HYPOKINESIA, SEVERE LV DYSFUNCTION
NO H/O OTHOPNEA, PAROXYSMAL NOCTURNAL DYSPNOEA , PALPITATIONS, CHEST PAIN,
GIDDINESS
PAST ILLNESS:
NOT A KNOWN CASE OF HTN, DM, CVA, ASTHMA,EPILEPSY, TB
PERSONAL HISTORY:
DIET- MIXED
APPETITE- DECREASED
BOWEL AND BLADDER MOVEMENTS- REGULAR
SLEEP- ADEQUATE
ADDICTIONS- NONE
ON EXAMINATION AT ADMISSION:
PATEINT IS CONSCIOUS, COHERENT, COOPERATIVE
NO PALLOR ICTERUS, CYANOSIS, CLUBBING, LYMPHADENOPATHY, PEDAL EDEMA
BP- 90/50MMHG
PR- 85BPM
RR-24CPM
SPO2- 88%@RA 95% ON 8L OF O2
GRBS- 126MG/DL
CVS-S1 S2 +
RS- BAE+, B/L BASAL CREPTS HEARD
PA- SOFT NON TENDER
CNS- NFD
ON EXAMINATION AT DISCHARGE:
PATEINT IS CONSCIOUS, COHERENT, COOPERATIVE
BP- 90/50MMHG
Page-3
PR- 72BPM
SPO2- 98%@RA
GRBS- 82MG/DL
CVS-S1 S2 +
RS- BAE+, B/L BASAL CREPTS HEARD, RT IAA CREPTS +, BRONCHIAL BREATH SOUNDS +
PA- SOFT NON TENDER
CNS- NFD
BRIEF COURSE IN HOSPITAL-ON DAY 1 PATIENT PRESENTED WITH ABOVE COMPLAINTS
WAS INITIALLY CONSCIOUS, COHERENT AND COOPERATIVE .AT THE TIME OF ADMISSION
HER BP WAS 90/50 WITH OUTSIDE ECHO SHOWING CAD(LAD TERRITORY) WITH GLOBAL
HYPOKINESIA AND SEVERE LV DYSFUNCTION.THEN DIURETICS AND ANTIPLATELETS
WERE STARTED.MONITORING HER BP AND CARDIOLOGY CONSULTATION WERE TAKEN ON
3/2/23 I/V/O CORONARY ARTERY DISEASE AND CARDIOLOGIST ADVICED INJ.HEPARIN 4000
IU/IV/BD AND TAB.CAVERDILOL 3.125 MG WAS ADVICED AND ADVICE FOLLOWED AND HER
SODIUM AND POTASSIUM LEVELS FOUND TO BE LOW AND ORAL POTASSIUM
Supplementation WAS GIVEN AND HER TRUE HYPONATREMIA WAS ATTRIBUTED TO
?SIADH. AS HER CHEST X RAY SHOWED MIDDLE LOBE CAVITY OF RT.LUNG USG CHEST
WAS DONE WHICH SHOWED BILATERAL PLEURAL EFFUSION(TAP NOT DONE).ON 3/2/23
OPTHALMOLOGY REFERRAL WAS DONE I/V/O RAISED ICT FEATURES AND ADVICE
FOLLOWED ON 4/2/23 PULMONOLOGY REFERRAL WAS DONE I/V/O X RAY CHANGES AND
ADVICE FOLLOWED.ON 3/2/23 PT MEAN ARTERIAL PRESSURE WAS NOT MAINTAINED AND
WAS STARTED ON INJ.NORAD AND ADJUSTED ACCORDING TO HER BP .X RAY REPORTING
WAS DONE AND SHOWED BILATERAL LUNG CONSOLIDATION WITH MILD
CARDIOMEGALY.PATIENT WAS IRRITABLE DUE TO ?ICU PSYCHOSIS AND ANXIOLYTICS
WERE GIVEN.NEXT DAY AS HER MEAN ARTERIAL PRESSURE WAS NOT MAINTAINED
INJ.DOBUTAMINE 250 MCG IN 50ML NS WAS STARTED AND TAPERED AS HER BP
IMPROVED.PATIENT CONDITION IMPROVED AND
DISCHARGED IN A HEMODYNAMICALLY STABLE CONDITION
Investigation
USG ABDOMEN-NAD
USG CHEST RIGHT MILD PLEURAL EFFUSION
HEMOGRAM ON 3/2/23
HB- 10.7 GM/DL
Page-4
TLC- 10,300 CELLS/CUMM
PLATELETS- 3.77 LAKHS/CUMM
N/L/E/M/B- 74/16/01/09/00
PCV- 32.3 VOL%
MCV- 85.7 FL
MCH- 28.4 PG
MCHC- 33.1%
RBC- 3.77
IMPRESSION- NORMOCYTIC NORMOCHROMIC BLOOD PICTURE
HEMOGRAM ON 8/2/23
HB- 9.9 GM/DL
TLC- 5700 CELLS/CUMM
PLATELETS- 3.27 LAKHS/CUMM
N/L/E/M/B- 57/26/02/15/00
PCV- 31.4 VOL%
MCV- 88 FL
MCH- 27.7 PG
MCHC- 31.5%
RBC- 3.57
IMPRESSION- NORMOCYTIC NORMOCHROMIC ANEMIA WITH MONOCYTOSIS
2DECHOESD- 5.44CMS
EDD- 6.3CM
DPW- 1CM
EF- 30%
FS- 15%
SEVERETR WITH PAH, MILD MR/AR
GLOBAL HYPOKINETIC
NO AS/MS
SCLEROTIC AV
MODERATE LV DYSFUNCTION
NO DIASTOLIC DYSFUNCTION
Page-5
REVIEW 2D ECHO ON 6/2/23
GLOBAL HYPOKINETIC
MODERATE TR WITH PAH, MILD MR, MODERATE AR
NO AS/MS, SCLEROTIC AV
EF=30
MODERATE LV DYSFUNCTION
NO DIASTOLIC DYSFUNCTION
IVC SIZE COLLAPSING
MILD DILATED LA/LV
DILATED RA.RV
NO PAH/PE
Treatment Given(Enter only Generic Name)
T. ECOSPRIN GOLD PO HS [75/75/10 MG]
T. MET XL 25MG PO OD
INJ LASIX 20MG IV BD
INJ NORAD DS 2AMP IN 46ML NS IV @ 6ML/HR
FLUID RESTRICTION
O2 SUPLEMENTATION TO MAINTAIN SPO2>94%
Advice at Discharge
T. ECOSPRIN GOLD 75/75/10 MG PO/HS
T.DYTOR 5MG PO/OD 9AM--*--*
T.CARDIVAS 3.125MG PO/OD 8AM--*--*
FLUID RESTRICTION <1LTR/DAY
Follow Up
REVIEW TO GM OP AFTER 1 WEEK/SOS
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR
ATTEND EMERGENCY DEPARTMENT.
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact:
For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed
and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been
explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date
Date: 8/2/23
Ward: MEDICAL WARD
Unit:IV
The second admission one month later 21-28 March 2023:
This author just realised that the PaJR discussion pasted above after the first admission actually took place in the second admission in a second PaJR group as the second team changed and were unaware of the previous team's approach. Altered sensorium was a more dominant feature in the second admission!
Following which the PaJR discussion took place as already pasted above. Pasting the concluding part of the discussion where there's an interjection by the patient's relative thanking the team for their care (actually pasted earlier above).
23/03/23, 11:55 - ~ f PRES is still unclear. Three hypotheses have been proposed till now, which include (i) Cerebral vasoconstriction causing subsequent infarcts in the brain, (ii) Failure of cerebral autoregulation with vasogenic edema, and (iii) Endothelial damage with blood–brain barrier disruption further leading to fluid and protein transudation in the brain. The distinct imaging patterns in PRES are represented in Table Table22 [5]. The reversible nature of PRES has been challenged recently based on new reports of permanent neurological impairment and mortality reaching 15%.
hypertension associated or drug-induced PRES, the effective therapy includes withdrawal of offending agent, immediate control of blood pressure, anti-convulsive therapy and temporary renal replacement therapy (hemodialysis/peritoneal dialysis) if revite link
29/03/23, 16:28 - Dr Rakesh Biswas Sir HOD changed the group name from "88F CAD Cardiogenic shock Cerebral infarct hyponatremia altered sensorium Telengana PaJR" to "88F Recurrent hypog Cardiogenic shock Cerebral infarct hyponat alt sen Telengana PaJR"
29/03/23, 16:18 - Dr Rakesh Biswas Sir HOD: IMG-20230329-WA0049.jpg (file attached)
This patient was admitted on 21st March and discharged on 28th March yesterday and there was no discussion around her current problems in her previous PaJR group!! @tm @tm
29/03/23, 16:21 - Dr Rakesh Biswas Sir HOD: Her current admission due to hypoglycemia and subsequent ordering of a test, morning serum cortisol that shows reduced values should ring a bell around the current 90M with hypoglycemia @tm ?
@tm Can you share the deidentified serum cortisol reports that were done from outside recently?
29/03/23, 16:24 - Dr Ajay Gen Med Pg: IMG-20230329-WA0048.jpg (file attached)
29/03/23, 16:24 - Dr Ajay Gen Med Pg: IMG-20230329-WA0047.jpg (file attached)
29/03/23, 16:24 - Dr Ajay Gen Med Pg: IMG-20230329-WA0046.jpg (file attached)
29/03/23, 17:59 - Dr Abhinaya, SR. joined using this group's invite link
29/03/23, 18:13 - Dr Aditya Gmed Pgy3 joined using this group's invite link
29/03/23, 18:29 - Dr Aditya Gmed Pgy3: Going out on a limb here - I still think that is a cavity (TB) and the patient has hypotension, Hyponatremia and hypoglycemia with hyperkalemia. Looking like an Addisonian crisis?
Assuming all these were considered already.
Second admission discharge summary (March 21-28 2023)
DEPARTMENT OF GENERAL-MEDICINE
DISCHARGE SUMMARY ***
Pay Type : Paying
Age/Gender : 89 Years/Female
Address :
Discharge Type: Relieved
Admission Date: 21/03/2023 08:15 PM
Name of Treating Faculty
Diagnosis at discharge:
RECURRENT HYPOGLYCEMIA [RESOLVING ] ? ADRENAL INSUFFICIENCY ? , AKI (PRERENAL)
ON CKD WITH HYPOVOLEMIC SHOCK SECONDARY TO ACUTE GASTROENTERITIS WITH
HEART FAILURE WITH PRESERVED EJECTION FRACTION OF 55% SECONDARY TO CAD
(OLD AWMI) WITH ANAEMIA (NORMOCYTIC NORMOCHROMIC)? NUTRITIONAL,CKD WITH
URINE CULTURE AND SENSITIVITY [ ESCHERICIA COLI SENSITIVE TO NITROFURANTOIN
AND FOSFOMYCIN]
Case History and Clinical Findings
PATIENT WAS BROUGHT TO THE CASUALITY ON 21/3/23 AT 7:57 PM WITH COMPLAINTS OF
-DECREASED SPEECH , SLURRED SPEECH , DROWSY SINCE MORNING
- LOOSE STOOLS SINCE YESTERDAY - 3 EPISODES
HISTORY OF PRESENTING ILLNESS-
PATIENT WAS APPARENTLY ASYMPTOMATIC TILL YESTERDAY THEN SHE DEVELOPED
LOOSE STOOLS , 3 EPISODES , WATERY IN CONSISTENCY , NON BLOOD STAINED , NON
FOUL SMELLING . PATIENT WAS FOUND UNCONSCIOUS , NOT RESPONDING TO VERBAL
COMMANDS AND IN ALTERED SENSORIUM
NO H/O WEAKNESS IN BOTH LIMBS AND NOW DEVELOPED HYPOGLYCEMIA WITH GRBS - 31
MG/DL
NO H/O INVOLUNTARY MOVEMENTS IN BOTH LIMBS
NO H/O FEVER , VOMITINGS , CHEST PAIN , SOB
PAST HISTORY -
K/C/O HEART FAILURE WITH MID RANGE EJECTION FRACTION 42 % SECONDARY TO
ANTERIOR WALL MI WITH PRE RENAL AKI WITH RIGHT LL CONSOLIDATION WITH URETHRAL
CARBUNCLE
CARDIO VASCULAR SYSTEM -
S1 , S2 HEARD
NO MURMURS
RESPIRATORY SYSTEM -
BILATERAL AIR ENTRY PRESENT
NORMAL VESICULAR BREATH SOUNDS PRESENT
ABDOMEN -
SHAPE OF ABDOMEN - SOFT , NON TENDER , BOWEL SOUNDS PRESENT
CENTRAL NERVOUS SYSTEM -
CONCIOUS , COHERENT , COOPERATIVE , WELL ORIENTED TO TIME, PLACE AND PERSON
NO ABNORMALITY DETECTED
COURSE IN THE HOSPITAL -
88 YEARS FEMALE PRESENTED WITH THE ABOVE MENTIONED COMPLAINTS TO THE
CASUALTY PATIENT WAS EVALUATED CLINICALLY AND WITH APPROPRIATE
INVESTIGATIONS WHICH REVEALED RECURRENT HYPOGLYCEMIA. PATIENT WAS GIVEN
25D INFUSION FOR 1 DAY AFTER WHICH THE PATIENT SUGAR STABILIZED AND
ENDOCRINOLOGIST CONSULTATION WAS TAKEN AND ADVICED FOR
1. SERUM CORTISOL
2. SERUM PEPTIDE
3. GROWTH HORMONE LEVELS
4. SMALL FREQUENT MEAL
5. MONITOR GRBS
PATIENT RECOVERED SYMPTOMATICALLY AND WAS DISCHARGED IN STABLE CONDITION
Page-3
Investigation
HEMOGRAM
HB- 7.9
TLC- 9900
NEU-73
LYM-19
PCV-26
MCV-86.7
MCH-26.3
MCHC--30.4
RBC-3.00
PLT-2.65
ULTRASOUND REPORT -
E/O 5-6 MM HYPERECHOIC FOCI NOTED IN CONTRACTED GALL BLADDER
2D ECHO -
EF-55
MODERATE AORTIC REGURGITATION , MILD TRICUSPID REGURGITATION WITH PAH; MILD
MR
NO RWMA NO AS/MS , SCLEROTIC AV
GOOD LV SYSTOLIC FUNCTION
DIASTOLIC DYSFUNCTION NO PE
Treatment Given(Enter only Generic Name)
1. IV FLUIDS NS @ 50 ML / HR
2. INJ CIPROFLOXACIN 500 MG IV/BD
3. INJ METROGYL 500ML IV/TID
4. INJ LASIX 20 MG IV/BD
8AM------------4PM
5. TAB ECOSPRIN GOLD 75/75/10 PO/OD AT 8PM
6. SYP LACTULOSE 15 ML PO/HS AT 8PM
7. INPUT / OUTPUT CHARTING
8. GRBS MONITORING 2 HRLY
Advice at Discharge
TAB LASIX 20MG PO/BD
Page-4
TAB ECOSPRIN GOLD 70/75/10 PO/HS
SYP LACTULOSE 15ML PO/HS
SACHET OF 1 FOSFOMYCIN IN GLASS OF WATER PO ONCE IN 3 DAYS [NEXT DOSE ON
30/3/23 AND NEXT DOSE ON 3/3/23]
Follow Up
REVIEW TO GENERAL MEDICINE OPD AFTER 7 DAYS
REVIEW SOS
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR
ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact:
For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed
and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been
explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date
Date:28/3/23
Ward:AMC
Unit:GENERAL MEDICINE - II
Dr Haripriya entrusted as PI for this project had to collate all her patient's data for final evaluation and analysis of all the patient outcomes in her project and she chose to start with this patient.
Thematic analysis conversations between PaJR team members:
Dyadic conversational transcripts between two project team members
25/06, 08:16] ALLM: Please share the learning points from this case point wise and divide them into
What was already known to you before your study
What was already known to the world before your study although you didn't know it
What was not known to the world before your study
[25/06, 09:40] Pushed Communicator 1N21: In this case she is a elderly female with no comorbidities came with fluctuations in her sensorium sir..
*Before my study* I thought that hyponatremia doesn't cause altered sensorium and hyponatremia is common in elderly people and there will be triggers for hyponatremia to present this way..
But *after my study(which is already known to the world)* I found out that, hyponatremia can cause altered sensorium (it can be fluctuating)in this patient,and it's most common in old age which is responsible for recurrent history of falls..
This article showed:
Hospitalised pts with hyponatremia
Total :100 number.
Elderly:30
Among this,20pts(67%)have no or non specific symptoms of hyponatremia and remaining 10(33%),altered sensorium without FND..
1 person (30%) is having iatrogenic cause for hyponatremia,and 5(17%),had underlying bacterial chest infection leading to hyponatremia....
In this patient,acute cough from 2 days has triggered her heart failure and to look for chest infection,PA view was ordered initially and later asked for lateral view,to look for middle lobe pathology,and the chest infection caused Hyponatremia in this female,adding to the study...
What am *trying to convey to the world* about this patient is patients with hyponatremia can present with altered sensorium (which is already known),but that sensorium need not to be constant and can be fluctuating altered sensorium as in this patient..
[25/06, 10:14] ALLM: I would be more interested to know about what you learned about the unique fluctuations of sensorium in this patient. What were the event triggers and timeline of her rising and falling sensorium? Can you share it graphically?
[25/06, 18:48] Pushed Communicator 1N21: I've shared my learning points sir
[25/06, 18:48] Pushed Communicator 1N21: Anything more in this case sir
[25/06, 19:09] Rakesh Biswas: Would be more interested to know about what you learned about the unique fluctuations of sensorium in this patient. What were the event triggers and timeline of her rising and falling sensorium? Can you share it graphically?
[25/06, 19:10] Pushed Communicator 1N21: Sir
How can I draw the timeline of events graphically sir
As you will be saying that,our discussion should be starting from the beginning (when the pt gets admitted)
The similar way,we discussed the case bedside sir.
There are lot more cases of mine discussed at the time of admission itself
[25/06, 19:11] ALLM : It's the patient timeline we regularly share in the form of soap notes in the fever chart
[25/06, 19:12] Pushed Communicator 1N21: Yes.
It's already there in the blog shared in the morning
[25/06, 19:13] ALLM: I didn't see the:
Event triggers and timeline of her rising and falling sensorium in relation to her sodium values
PaJR team based learning:
[26/06, 12:04] Sai Charan Kulkarni 2020 KIMS Pg: *Independent Ai Researcher Analysis of the Blog "Case Report Form in BEHR Blended EMR"*
*Introduction*
The blog post titled "Case Report Form in BEHR Blended EMR" discusses the integration and functionality of case report forms (CRFs) within the BEHR (Blended Electronic Health Record) system. It provides insights into the implementation, benefits, and potential challenges of using CRFs in a blended electronic medical records (EMR) environment.
*Thematic Analysis*
1. **Integration and Implementation**
- **Seamless Integration**: The BEHR system integrates CRFs to streamline data collection and patient management processes. This integration allows for real-time data entry and retrieval, which enhances clinical efficiency.
- **Customizable Templates**: The system supports customizable CRF templates, enabling healthcare providers to tailor forms to specific study requirements or clinical needs. This flexibility is crucial for accommodating various research and clinical scenarios.
2. **Benefits of CRFs in BEHR**
- **Enhanced Data Accuracy**: The use of CRFs within BEHR improves the accuracy of data collection by minimizing manual entry errors and ensuring standardized data capture.
- **Improved Patient Care**: Real-time data availability through BEHR allows for more informed clinical decisions, leading to better patient outcomes.
- **Facilitation of Clinical Research**: CRFs in BEHR support clinical research by providing a structured way to collect and analyze patient data, which is essential for observational studies and clinical trials.
3. **Challenges and Solutions**
- **User Training and Adaptation**: One challenge is ensuring that healthcare providers are adequately trained to use the new system. The blog suggests ongoing training and support to mitigate this issue.
- **Data Privacy and Security**: The integration of CRFs into an EMR system raises concerns about data privacy and security. The BEHR system addresses these concerns through robust encryption and access controls.
4. **Future Prospects**
- **Scalability**: The blog highlights the potential for scaling the BEHR system to accommodate larger datasets and more complex clinical studies.
- **Interoperability**: There is an emphasis on improving interoperability with other health information systems, which would facilitate more comprehensive data sharing and collaboration across different healthcare institutions.
*Conclusion*
The blog post provides a comprehensive overview of the integration of case report forms in the BEHR Blended EMR system, highlighting the benefits of enhanced data accuracy, improved patient care, and facilitation of clinical research. It also acknowledges the challenges of user training and data security, suggesting solutions such as ongoing education and robust security measures. The potential for scalability and improved interoperability positions the BEHR system as a promising tool for future healthcare and research applications.
[26/06, 12:11] Rakesh Biswas: 👏👏For the AI LLM
Not sure about the AI researcher 😅
[26/06, 12:15] Rakesh Biswas: Which LLM is this?
It has completely ignored the patient's outcomes and focused only on our novel system of EHR driven case reporting aka case report form (in short CRF) traditionally in patient driven clinical trials.
Nevertheless this is also an important theme to explore
[26/06, 12:34] Chandana KIMS 2020 SR: From this case report I understand that she was admitted two times.
Feb 2023 she was treated for HfrEF, Anterior wall MI, hyponatremia secondary to SIADH, hypokalemia and pneumonia
In 2nd admission the significant problem was altered sensorium secondary to ? Uremia ? Hypoxia with suspected ILD and hypotension when adrenal crisis was also considered.
I dint understand why PRES was considered.
Complexity of managing elderly female with altered sensorium with multiple complex etiologies and stressors such as hypoxia, uremia, pneumonia +\-sepsis, MI with heart failure, hypotension ,?neuro degeneration. All these making the cause of altered sensorium uncertain
[26/06, 12:47] Rakesh Biswas: Good point!
Can you scroll up to the PaJR data here and share why we (I guess it was me alone) thought of pres?
I have lost all past data in my new phone
[26/06, 12:50] Sai Charan Kulkarni 2020 KIMS Pg: Problem could be in the prompt. Just rephrased my prompt, this is what I get..
### Independent Researcher Clinical Analysis of Patient-Related Outcomes in the Blog "Case Report Form in BEHR Blended EMR"
#### Introduction
The blog post "Case Report Form in BEHR Blended EMR" discusses a detailed clinical case, including the patient's medical history, diagnostic procedures, treatment plan, and outcomes. This analysis focuses on patient-related outcomes, examining how the use of the BEHR system influenced the patient’s overall health, quality of life, and long-term prognosis.
#### Patient-Related Outcomes
1. **Health Outcomes**
- **Symptom Relief**: Post-treatment, the patient experienced significant relief from initial symptoms such as fatigue, shortness of breath, and chest pain. This was primarily due to effective coronary intervention and optimized medical management.
- **Control of Chronic Conditions**: Improved control of diabetes and hypertension was observed, with stabilized blood glucose and blood pressure levels. This outcome was facilitated by the BEHR system’s ability to track and adjust treatment plans in real-time.
2. **Quality of Life**
- **Physical Health**: The patient reported increased energy levels and physical capacity, allowing for greater engagement in daily activities and exercise. This improvement is attributed to the comprehensive management of their cardiovascular and metabolic conditions.
- **Mental Health**: Effective symptom management and reduced health-related anxiety contributed to better mental well-being. The patient benefited from continuous monitoring and support, which provided reassurance and improved overall mental health.
3. **Adherence and Compliance**
- **Medication Adherence**: The BEHR system’s real-time monitoring and reminders helped the patient adhere to their medication regimen, which is crucial for managing chronic conditions. Regular follow-ups and education reinforced the importance of compliance.
- **Lifestyle Changes**: The patient successfully implemented recommended lifestyle modifications, including dietary changes and increased physical activity. The support and education provided through the BEHR system played a significant role in sustaining these changes.
4. **Clinical Outcomes**
- **Cardiovascular Health**: Successful percutaneous coronary intervention (PCI) led to improved cardiovascular outcomes, with no significant post-operative complications. The patient's heart function stabilized, as evidenced by follow-up echocardiograms.
- **Long-Term Prognosis**: The patient’s long-term prognosis improved due to the combined effects of intervention, medication management, and lifestyle changes. Continuous monitoring via the BEHR system ensures that any potential issues can be promptly addressed, enhancing long-term health outcomes.
5. **Patient Satisfaction**
- **Engagement and Satisfaction**: The patient expressed high satisfaction with the care received, highlighting the ease of communication with healthcare providers and the support from the BEHR system. This engagement is crucial for sustained health improvements.
- **Empowerment**: Access to personal health data and educational resources empowered the patient to take an active role in managing their health, leading to better outcomes and increased satisfaction with the care process.
#### Conclusion
The clinical analysis of patient-related outcomes in the blog "Case Report Form in BEHR Blended EMR" demonstrates the significant positive impact of the BEHR system on the patient’s health, quality of life, and long-term prognosis. Enhanced symptom relief, better control of chronic conditions, improved mental and physical health, and high patient satisfaction are key outcomes observed. The integrated approach facilitated by the BEHR system underscores its potential to transform patient care through continuous support, accurate data collection, and effective treatment management.
[26/06, 12:52] Sai Charan Kulkarni 2020 KIMS Pg: Based on GPT 4 sir.
[26/06, 13:07] Rakesh Biswas: It's clearly hallucinating! 😅
AI hallucinations in PaJR thematic analysis is the title of our next paper
Themes emerging:
Elderly woman with altered sensorium
Clinical complexity:
Multiple comorbidities and organ failure
Diagnostic uncertainty:
Multiple possibilities for altered sensorium:
Metabolic (possible acute trigger):
Hypoglycemia
Hyponatremia
Hypoxia
Uremia
Structural (possible chronic vasculopathic process):
PRES
Neurodegenerative
Therapeutic uncertainty:
Each organ failure such as cardiac and vascular instability was tackled with standard of care
Epilogue and final outcome:
The patient reportedly died at home shortly after discharge from her second hospital admission