Case summary:
60M with metabolic syn phenotype, diabetes, hypertension 3 years and bilateral chronic knee osteoarthritis with recent PUO and cough since 1 month presented with sudden left upper limb monoparesis and shortness of breath. The serial chest X-rays were suggestive of cardiogenic pulmonary edema which was morphologically consistent with HFPeF on echocardiography showing LVH and LA dilation but a closer look at his HRCT revealed chronic cavitary lesions suggestive of tuberculosis and even as we spoke the CBNAAT for TB came positive and the MRI showed vasculopathy that could explain his sudden monoparesis. The confluence of CD and NCD has been a recurrent clinical complexity theme of late and in this instance the complexity was compounded by the fact that the stroke may have been either due to the CD or NCD driven vasculopathy although anatomical arterial territory of involvement may provide clues to differentiate further.
PaJR CBBLE transcripts:
Clinical metabolic phenotype:

Knee OA with fixed flexion deformity


Facial lesions with etiologic CD differentials ranging from viral chikungunya or tuberculosis

Paper based Timeline of events during hospital admission

Paper based treatment plan

[03/10, 16:54] : Chest X-ray On admission 60M

Day 2

Day 3






Dyadic with PG:
[03/10, 19:48] PG 2023: Sir can those rashes over his nose and cheek be of viral etiology
[03/10, 20:17] : Share an image
[03/10, 20:19] : Since when have they noticed these?
[03/10, 20:20] PG 2023: He is having fever since 7-10 days sir, since then they have noticed
[03/10, 20:21] PG 2023: Sir can it be of viral etiology, earlier you were mentioning about chikungunya plus dengue mutated virus?
[03/10, 20:22] : Yes
This means he has an acute viral over a chronic mycobacterial CD over a chronic NCD
[03/10, 20:25] PG 2023: Sir Can that rapid progression of chest xray changes are because of viral etiology?
[03/10, 21:11] : No it's because of heart failure pulmonary edema
[03/10, 21:11]: Viral ARDS wouldn't have recovered this quickly.
[03/10, 21:13] PG 2023: Sir does his HFpEF with EF 65 can cause that rapidly progressing pulmonary edema?
[03/10, 21:17] : Yes
Many similar patients here earlier and a project dissertation in progress for the same!
[04/10, 13:09] CBBLE moderator: One of the CD organisms inside 60M ICU 2 captured by the Microbiology tech
[04/10, 16:12] CBBLE moderator: https://www.researchgate.net/
[04/10, 16:17] CBBLE moderator: Please let us know the dermatologist inputs for this specific area
[05/10, 09:42] : 60M ICU
[05/10, 11:41] CBBLE moderator: Current ICU 60M with clinical complexity in an NCD plagued by multiple CDs: AFB 2+, suspected Chikungunya and a multi drug resistant E Coli that looks like harboring ESBL (as it's resistant to all cephalosporins) but not is not yet CRE (carbapenem resistant enterococci)
EMR summary:
Age/Gender : 60 Years/Male
Address :
Discharge Type: Relieved
Admission Date: 01/10/2024 03:54 PM
Diagnosis
TUBERCULAR VASCULITIS WITH ACUTE CVA LT HEMIPARESIS
Address :
Discharge Type: Relieved
Admission Date: 01/10/2024 03:54 PM
Diagnosis
TUBERCULAR VASCULITIS WITH ACUTE CVA LT HEMIPARESIS
Pulmonary tuberculosis
UTI
AKI ON CKD
MODERATE NON PROLIFERATIVE DIABETIC RETINOPATHY K/C/O DM II , HTN SINCE 3 YEARS
POST INFLAMMATORY HYPERPIGMENTATION WITH SENILE XEROSIS AND POST TRAUMATIC SCARS
Case History and Clinical Findings
C/O GIDDINESS SINCE 5 MONTHS
C/O WEAKNESS LEFT UPPER LIMB SINCE 5 DAYS
PT WAS APPARENTLY ASYMPTOMATIC TILL 5 MONTHS AGO THEN DEVELOPED GIDDINESS , INSIDIOUS IN ONSET GRADUALLY PROGRESSIVE
H/O FEVER 1 WEEK AGO SUBSIDED WITH MEDICATION SINCE 2 DAYS H/O SOB SINCE 2 DAYS
H/O Altered BEHAVIOUR SINCE 2 DAYS
H/O INABILITY TO COMB HIS HAIR BUTTON UNBUTTON HIS SHIRT HOLD OBJECTS WITH HIS LEFT HAND
H/O NECK PAIN SINCE 2 DAYS
NO H/O WEAKNESS OF OTHER LIMBS NO H/O DECREASED URINE OUTPUT
NO H/O ANY CRANIAL NERVE INVOLVEMENT
NO H/O TINGLING NUMBNESS OF BOTH LOWER LIMBS SINCE 3 Months NO H/O INVOLUNTARY MOVEMENTS OF BOTH UPPER AND LOWER LIMBS
UTI
AKI ON CKD
MODERATE NON PROLIFERATIVE DIABETIC RETINOPATHY K/C/O DM II , HTN SINCE 3 YEARS
POST INFLAMMATORY HYPERPIGMENTATION WITH SENILE XEROSIS AND POST TRAUMATIC SCARS
Case History and Clinical Findings
C/O GIDDINESS SINCE 5 MONTHS
C/O WEAKNESS LEFT UPPER LIMB SINCE 5 DAYS
PT WAS APPARENTLY ASYMPTOMATIC TILL 5 MONTHS AGO THEN DEVELOPED GIDDINESS , INSIDIOUS IN ONSET GRADUALLY PROGRESSIVE
H/O FEVER 1 WEEK AGO SUBSIDED WITH MEDICATION SINCE 2 DAYS H/O SOB SINCE 2 DAYS
H/O Altered BEHAVIOUR SINCE 2 DAYS
H/O INABILITY TO COMB HIS HAIR BUTTON UNBUTTON HIS SHIRT HOLD OBJECTS WITH HIS LEFT HAND
H/O NECK PAIN SINCE 2 DAYS
NO H/O WEAKNESS OF OTHER LIMBS NO H/O DECREASED URINE OUTPUT
NO H/O ANY CRANIAL NERVE INVOLVEMENT
NO H/O TINGLING NUMBNESS OF BOTH LOWER LIMBS SINCE 3 Months NO H/O INVOLUNTARY MOVEMENTS OF BOTH UPPER AND LOWER LIMBS
PAST HISTORY:
K/C/O CKD SINCE 10 YRS HEMODIALYSIS DONE 8 MONTHS AGO
K/C/O DM2 SINCE 3 YRS ON TAB.GLIMI PO/OD 1/2-X-X K/C/O HTN SINCE 3 YRS ON Unknown MEDICATION
H/O CATARACT SURGERY TO RIGHT EYE WIH NO IMPROVEMENT IN VISION POST SURGERY PERSONAL HISTORY:
GENERAL EXAMINATION:
NO PALLOR ICTERUS CYANOSIS CLUBBING LYMPHADENOPATHY EDEMA + PITTING TYPE EXTENDING UPTO KNEE
BP: 110/70 MMHG PR:100 BPM
RR: 16 CPM
TEMPERATURE: 100 F
SPO2: 98 %
CVS: NO THRILLS, S1S2 +, NO MURMURS RS: BAE+,NVBS
PER ABDOMEN:
SOFT , NON TENDER CNS :NFND
MOTOR SYSTEM;
RIGHT LEFT
TONE UL-N LL-N Decreased LL-N POWER UL-5/5 LL-5/5 UL-3/5 LL- 5/5 HAND GRIP N LOST
ON 3/10/24 OPHTHALMOLOGY REFERAL WAS DONE I/V/O FUNDUS EXAMINATION FOR RETINOPATHY CHANGES AND RAISED ICT FEATURES AND IMPRESSION GIVEN AS MODERATE NON PROLIFERATIVE DIABETIC RETINOPATHY CHANGES NOTED AND NO RAISED ICT CHANGES AS OF NOW.
ON 3/10/24 PULMO REFERAL WAS DONE I/V/O B/L LOWER LOBE PNEUMONIA AND ARDS AND ADVISED TAB.ISONIAZ 300MG PO/OD /BBF,TAB.RIFAMPICIN 600MG PO/OD/BBF,TAB PYRIZINAMIDE 1500MQ PO/THRICE WEEKLY/BBF,TAB.ETHAMBUTOL 900MG PO/THRICE WEEKLY,TAB.BENADON 40MG PO/OD,SYP.ASCORIL LS 2TSP PO/TID,CHEST PHYSIOTHERAPY
ON 4/10/24 DERMA REFERAL WAS DONE I/V/O ANNULAR LESIONS OVER B/L LOWER LIMBS AND EROSIONS , HYPERPIGMENTATION AROUND NOSE AND ADVISED LIQUID PARAFFIN L/A BD OVER BOTH LEGS FOR 2 WEEKS AND T-BACT OINTMENT L/A BD OVER RAW AREAS FOR 1 WEEK.
COURSE IN THE HOSPITAL: 60YR OLD MALE K/C/O TYPE II DM,HTN SINCE 3 YRS, K/C/O CKD, S/P 10 SESSIONS HEMODIALYSIS,LAST SESSION 8 MONTHS BACK, CAME WITH CHEIF COMPLAINTS OF FEVER,COUGH,COLD SINCE 10 DAYS, WEAKNESS OF LEFT UPPER LIMB SINCE 2 DAYS. VITALS AT PRESENTATION: BP: 80/50 MM HG, PR: 72 BPM, R: 18 CPM, SPO2
:98% @ RA. O/E HYPOTONIA PRESENT IN LEFT UPPERLIMB WITH POWER 4/5 IN LEFT UPPER LIMB AND LOWER LIMB, EXTENSOR PLANTAR ON LEFT SIDE . ON AUSCULTATION Crept Present IN B/L IAA,ISA,MA. MRI BRAIN SHOWED MULTIPLE TINY TO SMALL INFARCTS Involving CORTEX AND SUBCORTICAL WHITE MATTER OF B/L PARIETAL LOBES, HRCT CHEST SHOWED MODERATE CYSTIC BRONCHIECTASIS WITH INTERVENING LUNG PARENCHYMAL FIBROSIS SEEN IN THE RIGHT Upper Lobe ANTERIOR SEGMENT AND RIGHT MIDDLE LOBE.SMALL THICK WALLED CAVITORY LESION IN RIGHT LOWER LOBE LATERAL BASAL SEGMENT.MULTIPLE OTHER PATCHY AREAS OF CONSOLIDATION IN BILATERAL LUNGS.MULTIPLE SUBCENTRIMETRIC MEDIASTINAL LYMPH NODES. SPUTUM FOR TRUNAAT SHOWED MTB, RIFAMPICIN SENSITIVE AND SMEAR SHOWED AFB BACILLI. DIAGNOSED AS TUBERCULAR VASCULITIS WITH ACUTE CVA LT HEMIPARESIS, SEPSIS SECONDARY TO TUBERCULAR BRONCHIECTASIS, AKI ON CKD , MODERATE NON PROLIFERATIVE DIABETIC RETINOPATHY, K/C/O DM II , HTN SINCE 3 YEARS.TREATED WITH IONOTROPES I/V/O SEPTIC SHOCK , IV FLUIDS, ANTIBIOTICS, ANTIPYRETICS, STEROIDS. STARTED ON ATT ON 4/10/24 WITH HRZE REGIMEN AND OTHER SUPPORTIVE TREATMENT. PATIENT WAS IMPROVED CLINICALLY AND DISCHARGED IN HEMODYNAMICALLY STABLE CONDITION.
Investigation
HBsAg-RAPIDNegative Anti HCV Antibodies - RAPIDNon Reactive COMPLETE URINE EXAMINATION (CUE)COLOURPale yellowAPPEARANCEClearREACTIONA
mg/dl42-12 mg/dlCREATININE2.5 mg/dl1.3-0.9 mg/dlURIC ACID4.7 mmol/L7.2-3.5 mmol/LCALCIUM10.0 mg/dl10.2-8.6 mg/dlPHOSPHOROUS3.8 mg/dl4.5-2.5 mg/dlSODIUM129 mmol/L145-136 mmol/LPOTASSIUM3.9 mmol/L.5.1-3.5 mmol/L.CHLORIDE103 mmol/L98-107 mmol/LLIVER FUNCTION TEST (LFT) Total Bilurubin0.90 mg/dl1-0 mg/dlDirect Bilurubin0.19 mg/dl0.2-0.0 mg/dlSGOT(AST)15 IU/L35-0 IU/LSGPT(ALT)10 IU/L45-0 IU/LALKALINE PHOSPHATASE160 IU/L119-56 IU/LTOTAL PROTEINS6.9 gm/dl8.3-6.4 gm/dlALBUMIN2.3 gm/dl4.6-3.2 gm/dlA/G RATIO0.53COMPLETE URINE EXAMINATION (CUE) COLOURPale yellowAPPEARANCEClearREACTIONA
mg/dl42-12 mg/dlCREATININE2.4 mg/dl1.3-0.9 mg/dlURIC ACID5.0 mmol/L7.2-3.5 mmol/LCALCIUM10.0 mg/dl10.2-8.6 mg/dlPHOSPHOROUS4.2 mg/dl4.5-2.5 mg/dlSODIUM135 mmol/L145-136 mmol/LPOTASSIUM4.0 mmol/L.5.1-3.5 mmol/L.CHLORIDE101 mmol/L98-107 mmol/LRFT UREA68 mg/dl42-12 mg/dlCREATININE2.0 mg/dl1.3-0.9 mg/dlURIC ACID3.7 mmol/L7.2-3.5 mmol/LCALCIUM9.6 mg/dl10.2-8.6 mg/dlPHOSPHOROUS3.4 mg/dl4.5-2.5 mg/dlSODIUM134 mmol/L145-136 mmol/LPOTASSIUM3.6 mmol/L.5.1-3.5 mmol/L.CHLORIDE101 mmol/L98-107 mmol/LABG PH7.39PCO219.4PO291.6HCO311.
2D ECHO:
(ECCENTRIC TR) AND MODERATE TR WITH MILD PAH : TRIVIAL AR /MR NO RWMA ,NO AS/MS SCLEROTIC AV
GOOD LV SYSTOLIC FUNCTION GRADE I DIASTOLIC DYSFUNCTION NO LV CLOT
SPUTUM CULTURE
ZN STAIN AFB SEEN 2+
GRAM STAIN LESS THAN 10 EPITHELIAL CELLS GREATER THAN 24 PUS CELLS/ 4F
GRAM POSTIVE COOCCI IN PAIRS , CHAINS SEEN NORMAL OROPHARANGEAL FLORA GROWN
URINE CULTURE AND SENSITIVITY : E COLI ISOLATED
USG ABDOMEN AND PELVIS:(1/10/24) SLIGHTLY ALTERED ECHOTEXTURE OF LIVER
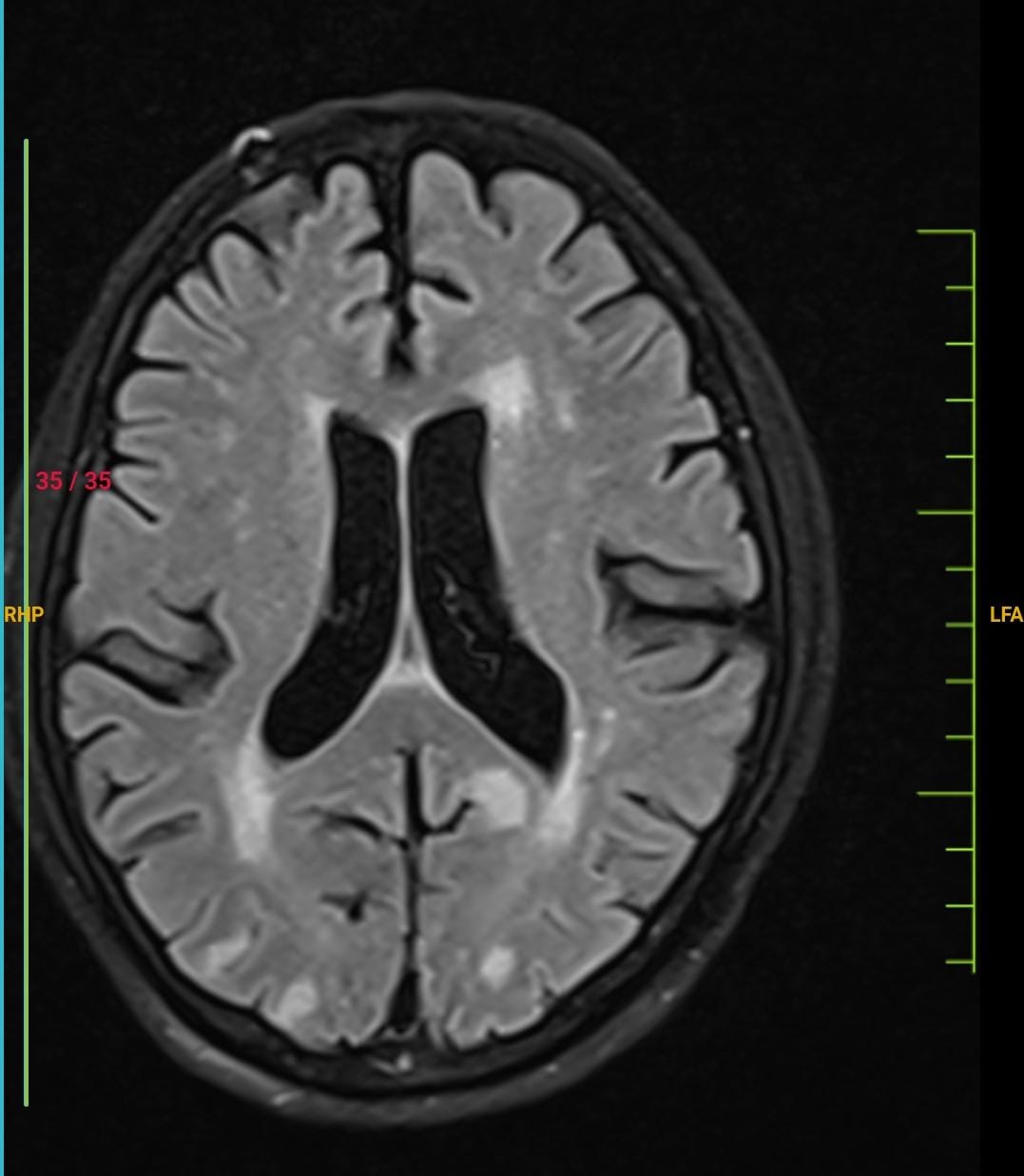
MRI BRAIN PLAIN (1/10/24): MULTIPLE TINY TO SMALL ACUTE INFARCTS INVOLVING THE CORTEX AND SUBCORTICAL WHITE MATTER OF BILATERAL PARIETAL LOBES.FEW TINY FOCI OF ACUTE INFARCTS Involving BILATERAL FRONTAL LOBES . FAZEKA'S GRADE II CHRONIC SMALL VESSELS WHITE MATTER ISCHEMIA.
MRI C SPINE WITH WHOLE SPINE SCREENING(1/10/24): CERVICAL SPONDYLOSIS AND DISC DEGENERATIVE CHANGES SEEN.
CT CHEST PLAIN: MODERATE CYSTIC BRONCHIECTASIS WITH INTERVENING LUNG PARENCHYMAL FIBROSIS SEEN IN THE RIGHT Upper Lobe ANTERIOR SEGMENT AND RIGHT MIDDLE LOBE.SMALL THICK WALLED CAVITORY LESION IN RIGHT LOWER LOBE LATERAL BASAL SEGMENT MEASURING 4 CM.AREA OF CONSOLIDATION INVOLVING LEFT UPPER LOBE ANTERIOR SEGMENT MEASURING APPROX 4.5 CM.MULTIPLE OTHER PATCHY AREAS OF CONSOLIDATION IN BILATERAL LUNGS. MULTIPLE SUBCENTRIMETRIC MEDIASTINAL LYMPH NODES.
Treatment Given(Enter only Generic Name)
1.IV FLUIDS 0.9 % NS @ 30 ML/HR INFUSION
2. INJ. NORADRENALINE 8 MG (4ML) IN 46 ML NS@2ML/HR INCREASE OR DECREASE TO MAINTAIN MAP-65MMHG
3. INJ.PIPTAZ 2.25GM IV/QID
4. INJ.PAN 40 IV/OD/BBF
5. INJ.HAI SC/TID PREMEAL ACC TO GRBS
6. TAB.ISONIAZID 300MG/PO/OD 7 AM/BBF
7. TAB.RIFAMPICIN 600MG/PO/OD 7 AM/BBF
8. TAB.PYRAZINAMIDE 1500MG/PO/OD 9 AM/BBF ALTERNATE DAYS
9. TAB.ETHAMBUTOL 900MG/PO/OD 9 AM/BBF ALTERNATE DAYS 10.TAB.BENADONE 40MG PO/OD
11. SYP.ASCORIL LS 15ML PO/TID
12. CHEST PHYSIOTHERAPY
13. TAB.PCM 650 MG PO/SOS
14. TAB.OROFERXT PO/OD/8 AM
15. NEPHRO LP PROTEIN POWDER 2 TABLESPOON IN GLASS OF WATER TWICE DAILY
16. TAB.ECOSPRIN 75+CLOPIDOGRIL 75+ATORVAS 20 PO/HS/9 PM
17. NEB WITH BUDOCORT AND IPRAVENT 8TH HRLY
18. LIQ PARAFFIN L/A BD
19. GRBS TO PROFILE MONITORING
20. I/O CHARTING
21. MONITOR VITALS HRLY
22. TAB.PREDNISOLONE 30 MG PO/OD AT 8AM
23. TAB.NITROFURANTOIN 50MG PO/BD
24. EGG WHITES PER DAY 25.TEPID SPONGING
26. SYP POTKLOR 15ML IN GLASS OF WATER PO/TID
27. INJ. KCL 1 AMP WITH 1 AMP MGSO4 IN 500ML NS OVER 4 HOURS
Advice at Discharge
TAB.ISONIAZID 300MG/PO/OD 7 AM/BBF TAB.RIFAMPICIN 600MG/PO/OD 7 AM/BBF
TAB.PYRAZINAMIDE 1500MG/PO/OD /BBF ALTERNATE DAYS TAB.ETHAMBUTOL 900MG/PO/OD /BBF ALTERNATE DAYS TAB.PREDNISOLONE 30 MG PO/OD
TAB.NITROFURANTOIN 50MG PO/BD FOR 5 DAYS TAB.BENADONE 40MG PO/OD
SYP.ASCORIL LS 15ML PO/TID FOR 5 DAYS
NEPHRO LP PROTEIN POWDER 2 TABLESPOON IN GLASS OF WATER TWICE DAILY LIQ PARAFFIN L/A BD
TAB.ECOSPRIN 75+CLOPIDOGRIL 75+ATORVAS 20 PO/HS TAB.PAN 40 MG PO/OD/BBFFOR 5 DAYS
TAB.ZOFER PO/ SOS EGG WHITES PER DAY
GRBS MONITORING AT HOME
Follow Up
REVIEW TO GM OPD AND PULMO OPD AFTER 1 WEEK
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date Date:07/10/2024 Ward:ICU
Unit:II
K/C/O CKD SINCE 10 YRS HEMODIALYSIS DONE 8 MONTHS AGO
K/C/O DM2 SINCE 3 YRS ON TAB.GLIMI PO/OD 1/2-X-X K/C/O HTN SINCE 3 YRS ON Unknown MEDICATION
H/O CATARACT SURGERY TO RIGHT EYE WIH NO IMPROVEMENT IN VISION POST SURGERY PERSONAL HISTORY:
GENERAL EXAMINATION:
NO PALLOR ICTERUS CYANOSIS CLUBBING LYMPHADENOPATHY EDEMA + PITTING TYPE EXTENDING UPTO KNEE
BP: 110/70 MMHG PR:100 BPM
RR: 16 CPM
TEMPERATURE: 100 F
SPO2: 98 %
CVS: NO THRILLS, S1S2 +, NO MURMURS RS: BAE+,NVBS
PER ABDOMEN:
SOFT , NON TENDER CNS :NFND
MOTOR SYSTEM;
RIGHT LEFT
TONE UL-N LL-N Decreased LL-N POWER UL-5/5 LL-5/5 UL-3/5 LL- 5/5 HAND GRIP N LOST
ON 3/10/24 OPHTHALMOLOGY REFERAL WAS DONE I/V/O FUNDUS EXAMINATION FOR RETINOPATHY CHANGES AND RAISED ICT FEATURES AND IMPRESSION GIVEN AS MODERATE NON PROLIFERATIVE DIABETIC RETINOPATHY CHANGES NOTED AND NO RAISED ICT CHANGES AS OF NOW.
ON 3/10/24 PULMO REFERAL WAS DONE I/V/O B/L LOWER LOBE PNEUMONIA AND ARDS AND ADVISED TAB.ISONIAZ 300MG PO/OD /BBF,TAB.RIFAMPICIN 600MG PO/OD/BBF,TAB PYRIZINAMIDE 1500MQ PO/THRICE WEEKLY/BBF,TAB.ETHAMBUTOL 900MG PO/THRICE WEEKLY,TAB.BENADON 40MG PO/OD,SYP.ASCORIL LS 2TSP PO/TID,CHEST PHYSIOTHERAPY
ON 4/10/24 DERMA REFERAL WAS DONE I/V/O ANNULAR LESIONS OVER B/L LOWER LIMBS AND EROSIONS , HYPERPIGMENTATION AROUND NOSE AND ADVISED LIQUID PARAFFIN L/A BD OVER BOTH LEGS FOR 2 WEEKS AND T-BACT OINTMENT L/A BD OVER RAW AREAS FOR 1 WEEK.
COURSE IN THE HOSPITAL: 60YR OLD MALE K/C/O TYPE II DM,HTN SINCE 3 YRS, K/C/O CKD, S/P 10 SESSIONS HEMODIALYSIS,LAST SESSION 8 MONTHS BACK, CAME WITH CHEIF COMPLAINTS OF FEVER,COUGH,COLD SINCE 10 DAYS, WEAKNESS OF LEFT UPPER LIMB SINCE 2 DAYS. VITALS AT PRESENTATION: BP: 80/50 MM HG, PR: 72 BPM, R: 18 CPM, SPO2
:98% @ RA. O/E HYPOTONIA PRESENT IN LEFT UPPERLIMB WITH POWER 4/5 IN LEFT UPPER LIMB AND LOWER LIMB, EXTENSOR PLANTAR ON LEFT SIDE . ON AUSCULTATION Crept Present IN B/L IAA,ISA,MA. MRI BRAIN SHOWED MULTIPLE TINY TO SMALL INFARCTS Involving CORTEX AND SUBCORTICAL WHITE MATTER OF B/L PARIETAL LOBES, HRCT CHEST SHOWED MODERATE CYSTIC BRONCHIECTASIS WITH INTERVENING LUNG PARENCHYMAL FIBROSIS SEEN IN THE RIGHT Upper Lobe ANTERIOR SEGMENT AND RIGHT MIDDLE LOBE.SMALL THICK WALLED CAVITORY LESION IN RIGHT LOWER LOBE LATERAL BASAL SEGMENT.MULTIPLE OTHER PATCHY AREAS OF CONSOLIDATION IN BILATERAL LUNGS.MULTIPLE SUBCENTRIMETRIC MEDIASTINAL LYMPH NODES. SPUTUM FOR TRUNAAT SHOWED MTB, RIFAMPICIN SENSITIVE AND SMEAR SHOWED AFB BACILLI. DIAGNOSED AS TUBERCULAR VASCULITIS WITH ACUTE CVA LT HEMIPARESIS, SEPSIS SECONDARY TO TUBERCULAR BRONCHIECTASIS, AKI ON CKD , MODERATE NON PROLIFERATIVE DIABETIC RETINOPATHY, K/C/O DM II , HTN SINCE 3 YEARS.TREATED WITH IONOTROPES I/V/O SEPTIC SHOCK , IV FLUIDS, ANTIBIOTICS, ANTIPYRETICS, STEROIDS. STARTED ON ATT ON 4/10/24 WITH HRZE REGIMEN AND OTHER SUPPORTIVE TREATMENT. PATIENT WAS IMPROVED CLINICALLY AND DISCHARGED IN HEMODYNAMICALLY STABLE CONDITION.
Investigation
HBsAg-RAPIDNegative Anti HCV Antibodies - RAPIDNon Reactive COMPLETE URINE EXAMINATION (CUE)COLOURPale yellowAPPEARANCEClearREACTIONA
mg/dl42-12 mg/dlCREATININE2.5 mg/dl1.3-0.9 mg/dlURIC ACID4.7 mmol/L7.2-3.5 mmol/LCALCIUM10.0 mg/dl10.2-8.6 mg/dlPHOSPHOROUS3.8 mg/dl4.5-2.5 mg/dlSODIUM129 mmol/L145-136 mmol/LPOTASSIUM3.9 mmol/L.5.1-3.5 mmol/L.CHLORIDE103 mmol/L98-107 mmol/LLIVER FUNCTION TEST (LFT) Total Bilurubin0.90 mg/dl1-0 mg/dlDirect Bilurubin0.19 mg/dl0.2-0.0 mg/dlSGOT(AST)15 IU/L35-0 IU/LSGPT(ALT)10 IU/L45-0 IU/LALKALINE PHOSPHATASE160 IU/L119-56 IU/LTOTAL PROTEINS6.9 gm/dl8.3-6.4 gm/dlALBUMIN2.3 gm/dl4.6-3.2 gm/dlA/G RATIO0.53COMPLETE URINE EXAMINATION (CUE) COLOURPale yellowAPPEARANCEClearREACTIONA
mg/dl42-12 mg/dlCREATININE2.4 mg/dl1.3-0.9 mg/dlURIC ACID5.0 mmol/L7.2-3.5 mmol/LCALCIUM10.0 mg/dl10.2-8.6 mg/dlPHOSPHOROUS4.2 mg/dl4.5-2.5 mg/dlSODIUM135 mmol/L145-136 mmol/LPOTASSIUM4.0 mmol/L.5.1-3.5 mmol/L.CHLORIDE101 mmol/L98-107 mmol/LRFT UREA68 mg/dl42-12 mg/dlCREATININE2.0 mg/dl1.3-0.9 mg/dlURIC ACID3.7 mmol/L7.2-3.5 mmol/LCALCIUM9.6 mg/dl10.2-8.6 mg/dlPHOSPHOROUS3.4 mg/dl4.5-2.5 mg/dlSODIUM134 mmol/L145-136 mmol/LPOTASSIUM3.6 mmol/L.5.1-3.5 mmol/L.CHLORIDE101 mmol/L98-107 mmol/LABG PH7.39PCO219.4PO291.6HCO311.
2D ECHO:
(ECCENTRIC TR) AND MODERATE TR WITH MILD PAH : TRIVIAL AR /MR NO RWMA ,NO AS/MS SCLEROTIC AV
GOOD LV SYSTOLIC FUNCTION GRADE I DIASTOLIC DYSFUNCTION NO LV CLOT
SPUTUM CULTURE
ZN STAIN AFB SEEN 2+
GRAM STAIN LESS THAN 10 EPITHELIAL CELLS GREATER THAN 24 PUS CELLS/ 4F
GRAM POSTIVE COOCCI IN PAIRS , CHAINS SEEN NORMAL OROPHARANGEAL FLORA GROWN
URINE CULTURE AND SENSITIVITY : E COLI ISOLATED
USG ABDOMEN AND PELVIS:(1/10/24) SLIGHTLY ALTERED ECHOTEXTURE OF LIVER
MRI BRAIN PLAIN (1/10/24): MULTIPLE TINY TO SMALL ACUTE INFARCTS INVOLVING THE CORTEX AND SUBCORTICAL WHITE MATTER OF BILATERAL PARIETAL LOBES.FEW TINY FOCI OF ACUTE INFARCTS Involving BILATERAL FRONTAL LOBES . FAZEKA'S GRADE II CHRONIC SMALL VESSELS WHITE MATTER ISCHEMIA.
MRI C SPINE WITH WHOLE SPINE SCREENING(1/10/24): CERVICAL SPONDYLOSIS AND DISC DEGENERATIVE CHANGES SEEN.
CT CHEST PLAIN: MODERATE CYSTIC BRONCHIECTASIS WITH INTERVENING LUNG PARENCHYMAL FIBROSIS SEEN IN THE RIGHT Upper Lobe ANTERIOR SEGMENT AND RIGHT MIDDLE LOBE.SMALL THICK WALLED CAVITORY LESION IN RIGHT LOWER LOBE LATERAL BASAL SEGMENT MEASURING 4 CM.AREA OF CONSOLIDATION INVOLVING LEFT UPPER LOBE ANTERIOR SEGMENT MEASURING APPROX 4.5 CM.MULTIPLE OTHER PATCHY AREAS OF CONSOLIDATION IN BILATERAL LUNGS. MULTIPLE SUBCENTRIMETRIC MEDIASTINAL LYMPH NODES.
Treatment Given(Enter only Generic Name)
1.IV FLUIDS 0.9 % NS @ 30 ML/HR INFUSION
2. INJ. NORADRENALINE 8 MG (4ML) IN 46 ML NS@2ML/HR INCREASE OR DECREASE TO MAINTAIN MAP-65MMHG
3. INJ.PIPTAZ 2.25GM IV/QID
4. INJ.PAN 40 IV/OD/BBF
5. INJ.HAI SC/TID PREMEAL ACC TO GRBS
6. TAB.ISONIAZID 300MG/PO/OD 7 AM/BBF
7. TAB.RIFAMPICIN 600MG/PO/OD 7 AM/BBF
8. TAB.PYRAZINAMIDE 1500MG/PO/OD 9 AM/BBF ALTERNATE DAYS
9. TAB.ETHAMBUTOL 900MG/PO/OD 9 AM/BBF ALTERNATE DAYS 10.TAB.BENADONE 40MG PO/OD
11. SYP.ASCORIL LS 15ML PO/TID
12. CHEST PHYSIOTHERAPY
13. TAB.PCM 650 MG PO/SOS
14. TAB.OROFERXT PO/OD/8 AM
15. NEPHRO LP PROTEIN POWDER 2 TABLESPOON IN GLASS OF WATER TWICE DAILY
16. TAB.ECOSPRIN 75+CLOPIDOGRIL 75+ATORVAS 20 PO/HS/9 PM
17. NEB WITH BUDOCORT AND IPRAVENT 8TH HRLY
18. LIQ PARAFFIN L/A BD
19. GRBS TO PROFILE MONITORING
20. I/O CHARTING
21. MONITOR VITALS HRLY
22. TAB.PREDNISOLONE 30 MG PO/OD AT 8AM
23. TAB.NITROFURANTOIN 50MG PO/BD
24. EGG WHITES PER DAY 25.TEPID SPONGING
26. SYP POTKLOR 15ML IN GLASS OF WATER PO/TID
27. INJ. KCL 1 AMP WITH 1 AMP MGSO4 IN 500ML NS OVER 4 HOURS
Advice at Discharge
TAB.ISONIAZID 300MG/PO/OD 7 AM/BBF TAB.RIFAMPICIN 600MG/PO/OD 7 AM/BBF
TAB.PYRAZINAMIDE 1500MG/PO/OD /BBF ALTERNATE DAYS TAB.ETHAMBUTOL 900MG/PO/OD /BBF ALTERNATE DAYS TAB.PREDNISOLONE 30 MG PO/OD
TAB.NITROFURANTOIN 50MG PO/BD FOR 5 DAYS TAB.BENADONE 40MG PO/OD
SYP.ASCORIL LS 15ML PO/TID FOR 5 DAYS
NEPHRO LP PROTEIN POWDER 2 TABLESPOON IN GLASS OF WATER TWICE DAILY LIQ PARAFFIN L/A BD
TAB.ECOSPRIN 75+CLOPIDOGRIL 75+ATORVAS 20 PO/HS TAB.PAN 40 MG PO/OD/BBFFOR 5 DAYS
TAB.ZOFER PO/ SOS EGG WHITES PER DAY
GRBS MONITORING AT HOME
Follow Up
REVIEW TO GM OPD AND PULMO OPD AFTER 1 WEEK
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date Date:07/10/2024 Ward:ICU
Unit:II











{kind=link}
{kind=link}